Kuper Willemijn F E, Oostendorp Marlies, van den Broek Brigitte T A, van Veghel Karin, Nonkes Lourens J P, Nieuwenhuis Edward E S, Fuchs Sabine A, Veenendaal Tineke, Klumperman Judith, Huisman Albert, Nierkens Stefan, van Hasselt Peter M
Department of Metabolic Diseases, Wilhelmina Children's Hospital University Medical Center Utrecht, Utrecht University Utrecht the Netherlands.
Department of Clinical Chemistry University Medical Center Utrecht Utrecht the Netherlands.
JIMD Rep. 2020 Jun 2;54(1):87-97. doi: 10.1002/jmd2.12128. eCollection 2020 Jul.
The CLN3 disease spectrum ranges from a childhood-onset neurodegenerative disorder to a retina-only disease. Given the lack of metabolic disease severity markers, it may be difficult to provide adequate counseling, particularly when novel genetic variants are identified. In this study, we assessed whether lymphocyte vacuolization, a well-known yet poorly explored characteristic of CLN3 disease, could serve as a measure of disease severity.
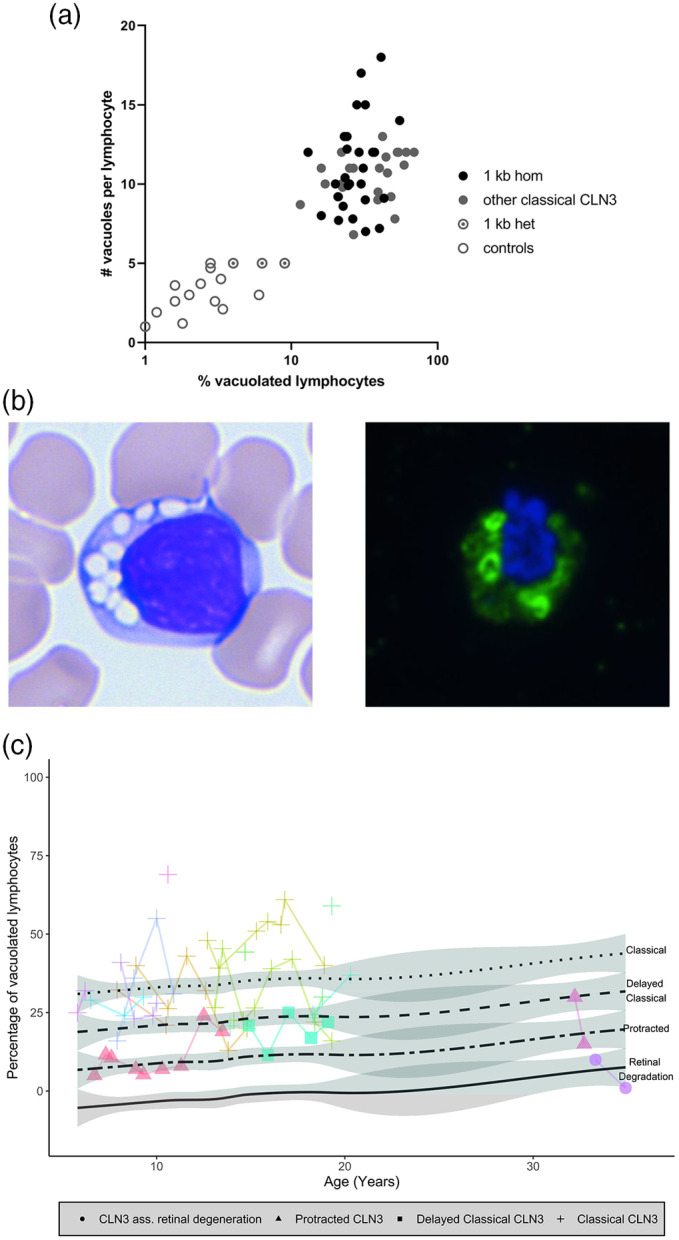
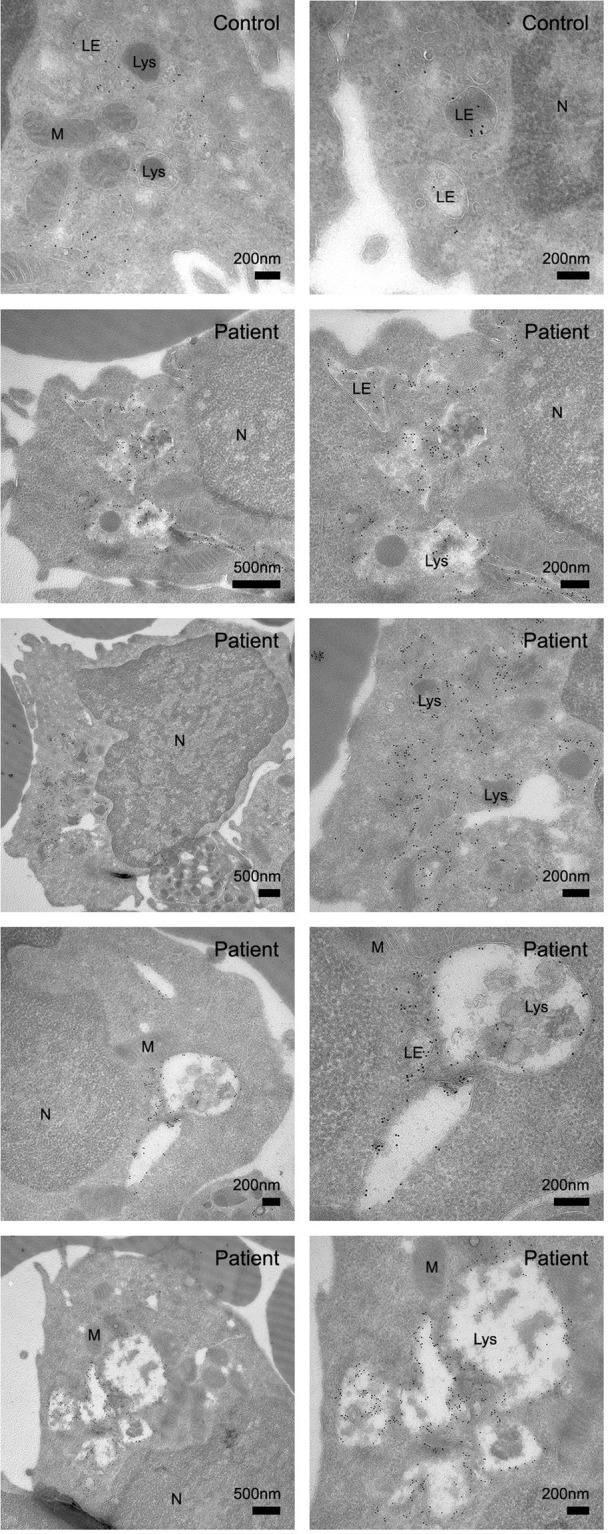
Peripheral blood obtained from healthy controls and CLN3 disease patients was used to assess lymphocyte vacuolization by (a) calculating the degree of vacuolization using light microscopy and (b) quantifying expression of lysosomal-associated membrane protein 1 (LAMP-1), using flow cytometry in lymphocyte subsets as well as a qualitative analysis using electron microscopy and ImageStream analysis.
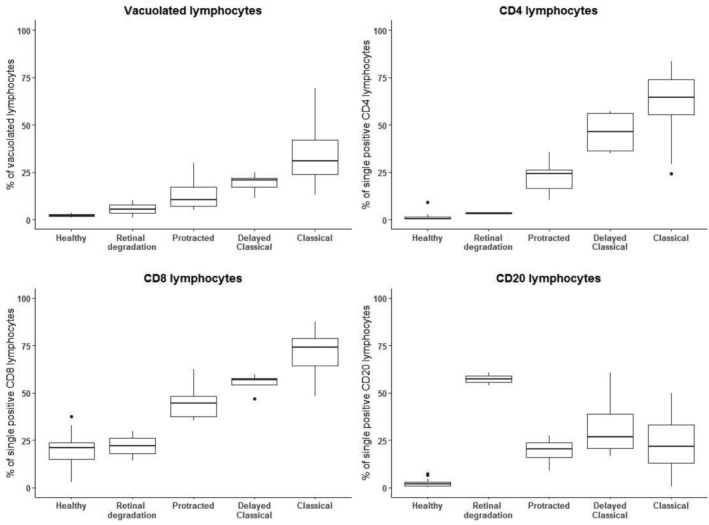
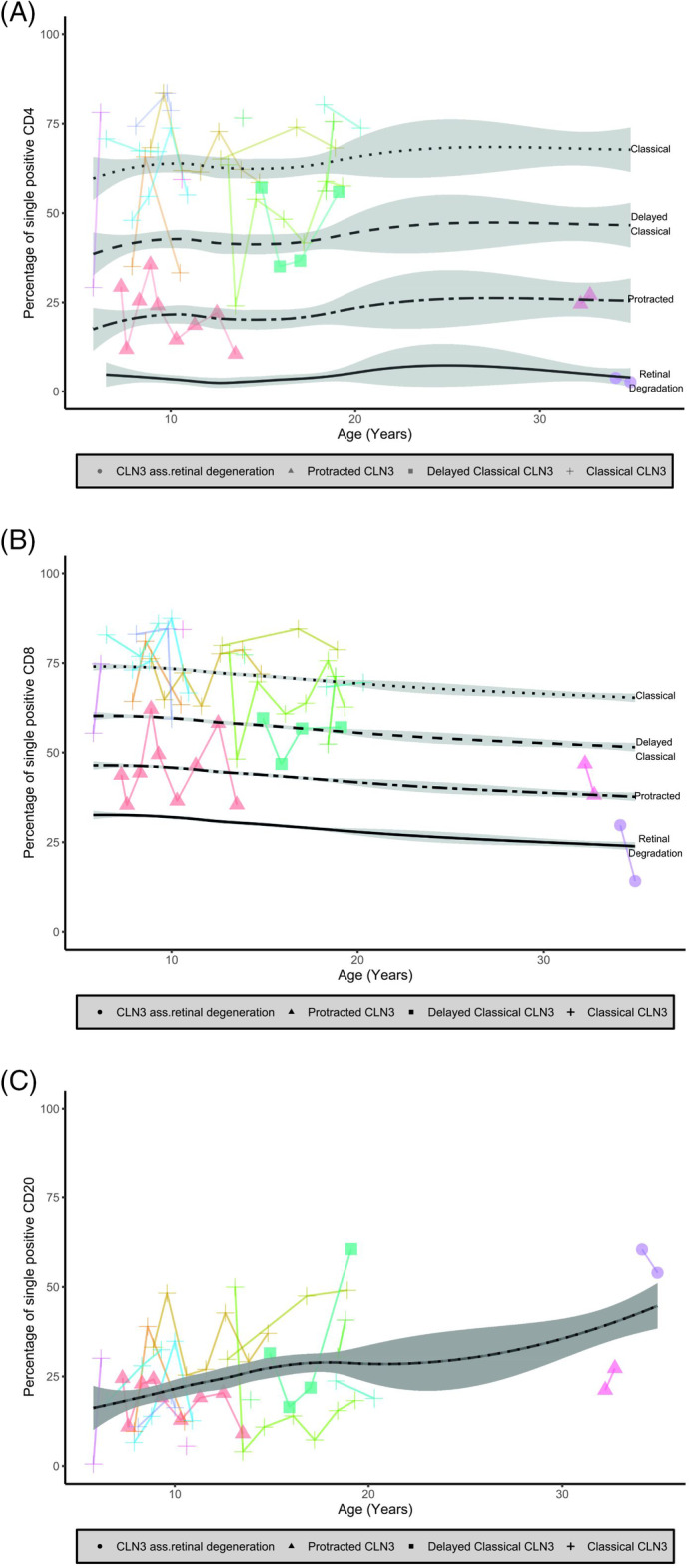
Quantifying lymphocyte vacuolization allowed to differentiate between CLN3 disease phenotypes ( = .0001). On immunofluorescence, classical CLN3 disease lymphocytes exhibited abundant vacuole-shaped LAMP-1 expression, suggesting the use of LAMP-1 as a proxy for lymphocyte vacuolization. Using flow cytometry in lymphocyte subsets, quantifying intracellular LAMP-1 expression additionally allowed to differentiate between infection and storage and to differentiate between CLN3 phenotypes even more in-depth revealing that intracellular LAMP-1 expression was most pronounced in T-cells of classical-protracted CLN3 disease while it was most pronounced in B-cells of "retina-only" CLN3 disease.
Lymphocyte vacuolization serves as a proxy for CLN3 disease severity. Quantifying vacuolization may help interpretation of novel genetic variants and provide an individualized readout for upcoming therapies.
CLN3病的疾病谱涵盖从儿童期起病的神经退行性疾病到仅累及视网膜的疾病。鉴于缺乏代谢性疾病严重程度标志物,可能难以提供充分的咨询,尤其是在鉴定出新的基因变异时。在本研究中,我们评估了淋巴细胞空泡化这一CLN3病的已知但研究较少的特征是否可作为疾病严重程度的一种衡量指标。
使用从健康对照和CLN3病患者获取的外周血,通过以下方式评估淋巴细胞空泡化:(a) 使用光学显微镜计算空泡化程度,以及(b) 使用流式细胞术在淋巴细胞亚群中定量溶酶体相关膜蛋白1 (LAMP-1) 的表达,并使用电子显微镜和ImageStream分析进行定性分析。
对淋巴细胞空泡化进行定量可区分CLN3病的不同表型(P = .0001)。在免疫荧光检查中,典型CLN3病淋巴细胞表现出丰富的空泡状LAMP-1表达,提示可将LAMP-1用作淋巴细胞空泡化的替代指标。在淋巴细胞亚群中使用流式细胞术,定量细胞内LAMP-1表达还可区分感染和蓄积情况,并更深入地区分CLN3病的不同表型,结果显示细胞内LAMP-1表达在经典迁延型CLN3病的T细胞中最为明显,而在“仅累及视网膜”型CLN3病的B细胞中最为明显。
淋巴细胞空泡化可作为CLN3病严重程度的替代指标。对空泡化进行定量可能有助于解释新的基因变异,并为即将开展的治疗提供个体化的评估结果。