Department of Surgery, Erasmus Medical Center, Rotterdam, The Netherlands.
Department of Pulmonary Medicine, Erasmus Medical Center, Rotterdam, The Netherlands.
J Immunother Cancer. 2020 Jul;8(2). doi: 10.1136/jitc-2020-000772.
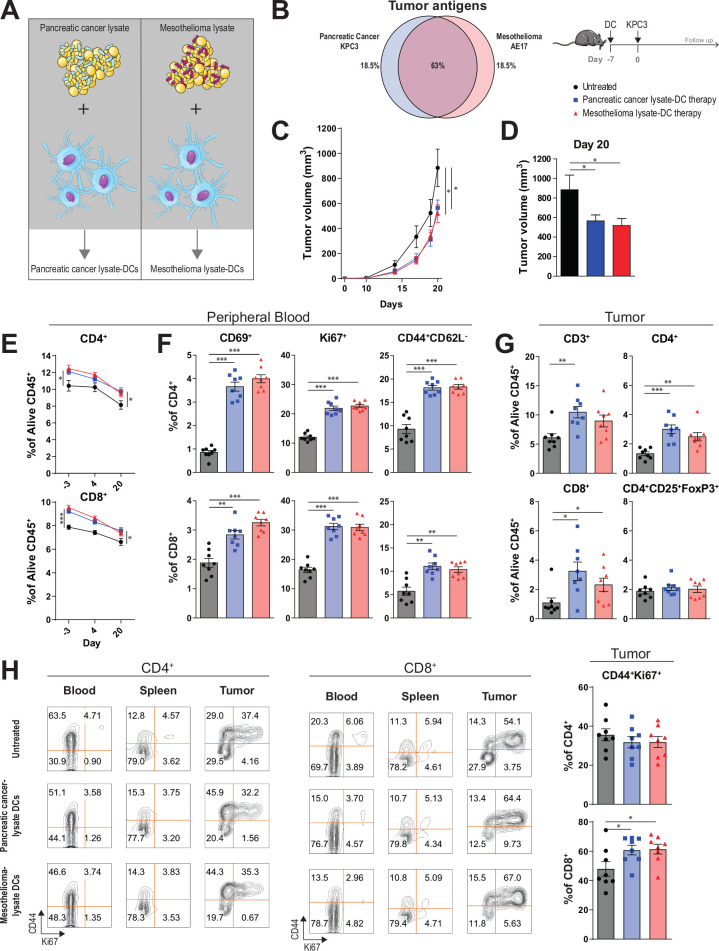
Pancreatic ductal adenocarcinoma (PDAC) is notoriously resistant to treatment including checkpoint-blockade immunotherapy. We hypothesized that a bimodal treatment approach consisting of dendritic cell (DC) vaccination to prime tumor-specific T cells, and a strategy to reprogram the desmoplastic tumor microenvironment (TME) would be needed to break tolerance to these pancreatic cancers. As a proof-of-concept, we investigated the efficacy of combined DC vaccination with CD40-agonistic antibodies in a poorly immunogenic murine model of PDAC. Based on the rationale that mesothelioma and pancreatic cancer share a number of tumor associated antigens, the DCs were loaded with either pancreatic or mesothelioma tumor lysates.
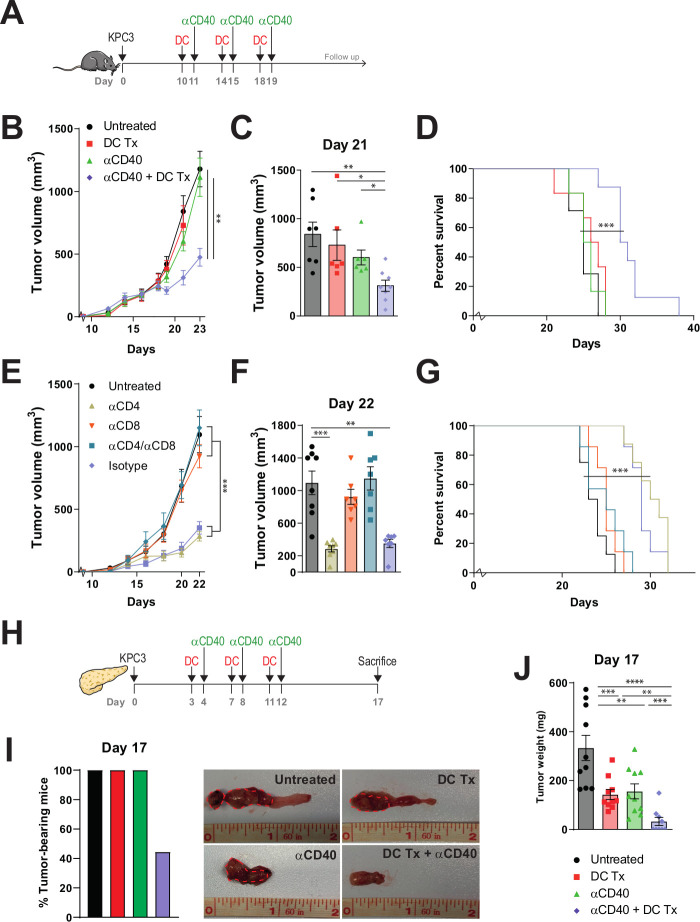
Immune-competent mice with subcutaneously or orthotopically growing KrasG12D/+;Trp53R172H/+;Pdx-1-Cre (KPC) PDAC tumors were vaccinated with syngeneic bone marrow-derived DCs loaded with either pancreatic cancer (KPC) or mesothelioma (AE17) lysate and consequently treated with FGK45 (CD40 agonist). Tumor progression was monitored and immune responses in TME and lymphoid organs were analyzed using multicolor flow cytometry and NanoString analyzes.
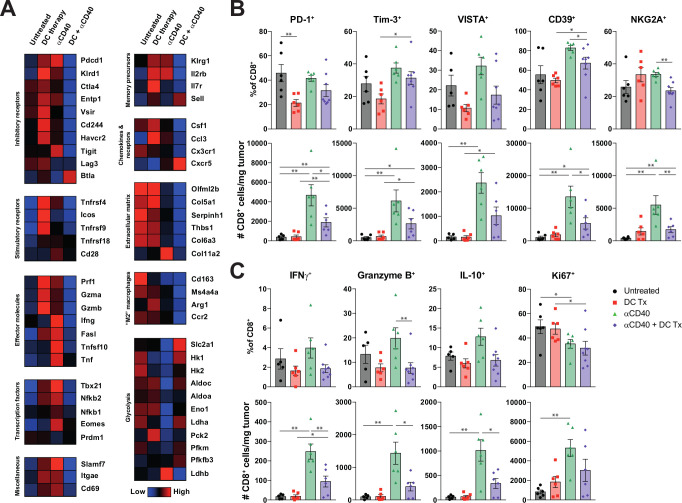
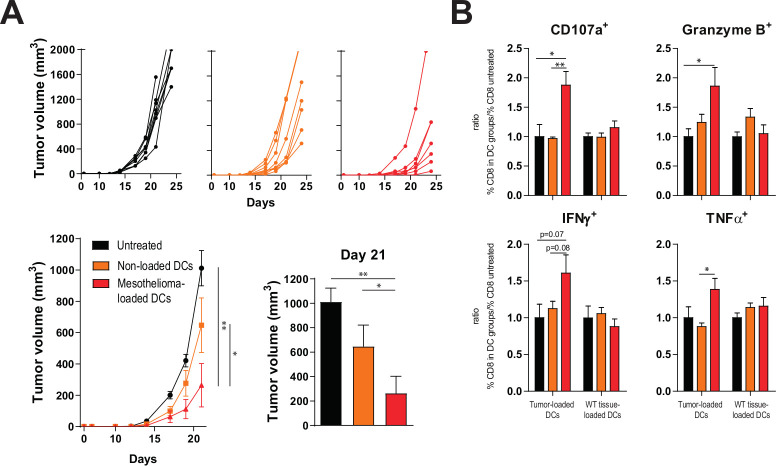
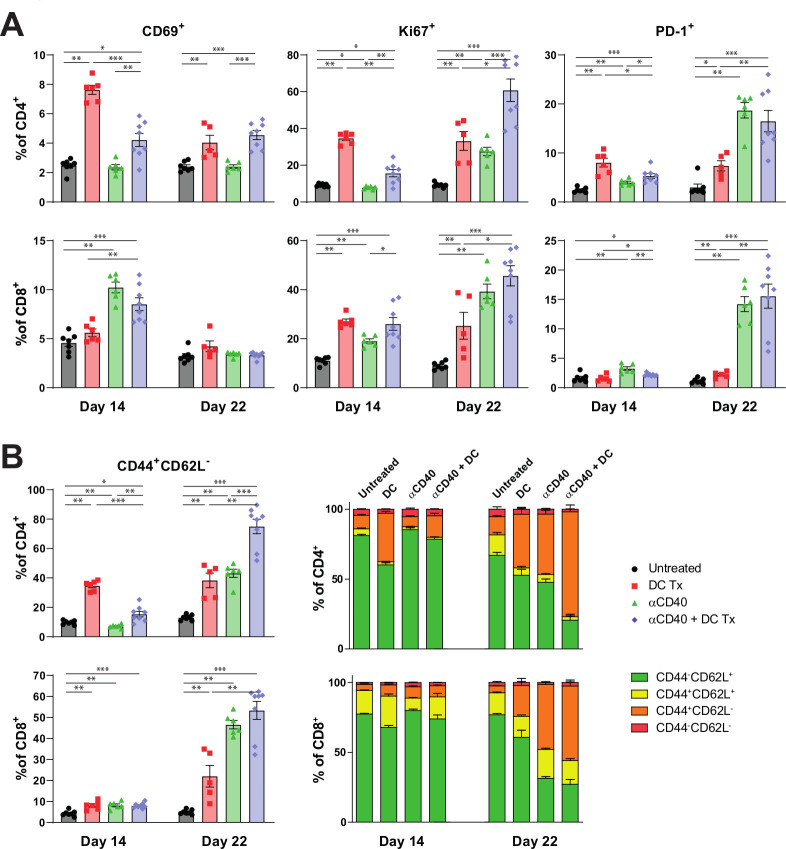
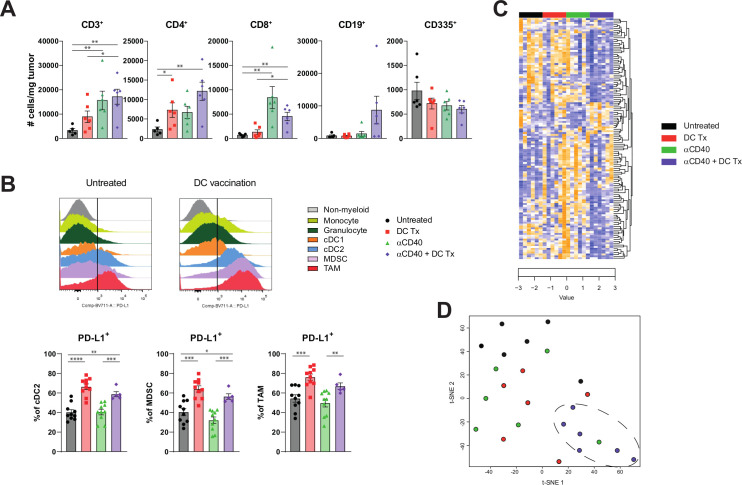
Mesothelioma-lysate loaded DCs generated cross-reactive tumor-antigen-specific T-cell responses to pancreatic cancer and induced delayed tumor outgrowth when provided as prophylactic vaccine. In established disease, combination with stimulating CD40 antibody was necessary to improve survival, while anti-CD40 alone was ineffective. Extensive analysis of the TME showed that anti-CD40 monotherapy did improve CD8 +T cell infiltration, but these essential effector cells displayed hallmarks of exhaustion, including PD-1, TIM-3 and NKG2A. Combination therapy induced a strong change in tumor transcriptome and mitigated the expression of inhibitory markers on CD8 +T cells.
These results demonstrate the potency of DC therapy in combination with CD40-stimulation for the treatment of pancreatic cancer and provide directions for near future clinical trials.
胰腺导管腺癌(PDAC)对治疗具有明显的耐药性,包括检查点阻断免疫治疗。我们假设,由树突状细胞(DC)疫苗接种来诱导肿瘤特异性 T 细胞,以及一种重新编程纤维瘤性肿瘤微环境(TME)的策略,将需要打破对这些胰腺癌的耐受性。作为概念验证,我们研究了 DC 疫苗接种联合 CD40 激动性抗体在胰腺导管腺癌的免疫原性低的小鼠模型中的疗效。基于间皮瘤和胰腺癌细胞共享许多肿瘤相关抗原的原理,用胰腺或间皮瘤肿瘤裂解物负载 DC。
用皮下或原位生长的 KrasG12D/+;Trp53R172H/+;Pdx-1-Cre(KPC)PDAC 肿瘤的免疫活性小鼠接种用胰腺癌细胞(KPC)或间皮瘤(AE17)裂解物负载的同源骨髓来源的 DC,随后用 FGK45(CD40 激动剂)治疗。监测肿瘤进展,并使用多色流式细胞术和 NanoString 分析分析 TME 和淋巴器官中的免疫反应。
用间皮瘤裂解物负载的 DC 产生了对胰腺癌细胞的交叉反应性肿瘤抗原特异性 T 细胞反应,并作为预防性疫苗提供时延迟了肿瘤生长。在已建立的疾病中,与刺激 CD40 抗体联合使用是改善生存所必需的,而单独使用抗 CD40 则无效。对 TME 的广泛分析表明,抗 CD40 单药治疗确实改善了 CD8+T 细胞浸润,但这些必需的效应细胞表现出衰竭的特征,包括 PD-1、TIM-3 和 NKG2A。联合治疗诱导了肿瘤转录组的强烈变化,并减轻了 CD8+T 细胞上抑制性标记物的表达。
这些结果证明了 DC 疗法联合 CD40 刺激在治疗胰腺癌方面的效力,并为即将进行的临床试验提供了方向。