Kormann Raphaël, Jacquot Audrey, Alla Asma, Corbel Alice, Koszutski Matthieu, Voirin Paul, Garcia Parrilla Matthieu, Bevilacqua Sybille, Schvoerer Evelyne, Gueant Jean-Louis, Namour Farès, Levy Bruno, Frimat Luc, Oussalah Abderrahim
Department of Nephrology, University of Lorraine, CHRU-Nancy, Vandoeuvre, France.
Department of Intensive Care Medicine, University of Lorraine, CHRU-Nancy, Vandoeuvre, France.
Clin Kidney J. 2020 Jun 8;13(3):362-370. doi: 10.1093/ckj/sfaa109. eCollection 2020 Jun.
Recent data have shown that severe acute respiratory syndrome coronavirus 2 can infect renal proximal tubular cells via Angiotensin Converting Enzyme 2 (ACE2) . Our objective was to determine whether Fanconi syndrome is a frequent clinical feature in coronavirus disease 2019 (COVID-19) patients.
A retrospective cohort of 42 laboratory-confirmed COVID-19 patients without history of kidney disease hospitalized in University Hospital of Nancy was investigated. Patients were admitted to the intensive care unit (ICU) ( = 28) or the Medical department ( = 14) and were screened at least once for four markers of proximal tubulopathy.
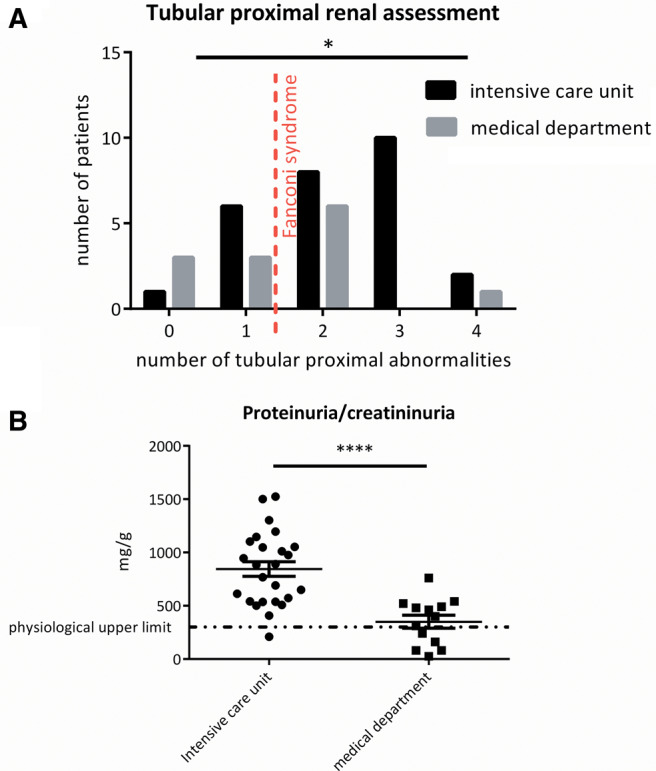
The mean (standard deviation) follow-up was 19.7 (±12.2) days. Of the patients, 75% (30/40) showed at least two proximal tubule abnormalities (incomplete Fanconi syndrome). The main disorders were proteinuria (88%, = 35), renal phosphate leak defined by renal phosphate threshold/glomerular filtration rate (TmPi/GFR) <0.77 (55%, = 22), hyperuricosuria (43%, = 17) and normoglycaemic glycosuria (30%, = 12). At the time of the first renal evaluation, ICU patients presented more frequent (96 versus 62%, P = 0.0095) and more severe (844 ± 343 versus 350 ± 221 mg/g, P = 0.0001) proteinuria, and a trend for an increased number of proximal tubule abnormalities (P = 0.038). During follow-up, they presented a lower nadir of serum phosphate [median (interquartile range) 0.68 (0.43-0.76) versus 0.77 (0.66-1.07) mmol/L, P = 0.044] and Acute kidney Injury (AKI) during the hospitalization (P = 0.045). Fanconi syndrome preceded severe AKI KDIGO Stages 2 and 3 in 88% (7/8) of patients. Proximal tubular abnormalities (such as proteinuria, TmPi/GFR and glycosuria in five, two and two patients, respectively) were not detected anymore in recovering patients before hospital discharge.
Incomplete Fanconi syndrome is highly frequent in COVID-19 patients and precedes AKI or disappears during the recovery phase.
最近的数据表明,严重急性呼吸综合征冠状病毒2可通过血管紧张素转换酶2(ACE2)感染肾近端小管细胞。我们的目的是确定范科尼综合征是否为2019冠状病毒病(COVID-19)患者常见的临床特征。
对南锡大学医院收治的42例实验室确诊的无肾脏疾病史的COVID-19患者进行回顾性队列研究。患者被收入重症监护病房(ICU)(n = 28)或内科病房(n = 14),并至少进行一次近端肾小管病变四项标志物的筛查。
平均(标准差)随访时间为19.7(±12.2)天。在这些患者中,75%(30/40)至少有两项近端小管异常(不完全性范科尼综合征)。主要异常包括蛋白尿(88%,n = 35)、以肾磷阈值/肾小球滤过率(TmPi/GFR)<0.77定义的肾磷泄漏(55%,n = 22)、高尿酸尿症(43%,n = 17)和正常血糖性糖尿(30%,n = 12)。在首次肾脏评估时,ICU患者蛋白尿更常见(96%对62%,P = 0.0095)且更严重(844±343对350±221mg/g,P = 0.0001),近端小管异常数量有增加趋势(P = 0.038)。在随访期间,他们血清磷的最低点更低[中位数(四分位间距)0.68(0.43 - 0.76)对0.77(0.66 - 1.07)mmol/L,P = 0.044],住院期间急性肾损伤(AKI)发生率更高(P = 0.045)。88%(7/8)的患者在发生严重AKI KDIGO 2期和3期之前出现范科尼综合征。在康复患者出院前未再检测到近端小管异常(如分别在5例、2例和2例患者中出现的蛋白尿、TmPi/GFR和糖尿)。
不完全性范科尼综合征在COVID-19患者中非常常见,在AKI之前出现或在恢复阶段消失。