University of Manitoba, Winnipeg, Manitoba, Canada.
Nova Scotia Health Authority and Dalhousie University, Halifax, Nova Scotia, Canada.
Arthritis Care Res (Hoboken). 2021 Jan;73(1):90-99. doi: 10.1002/acr.24386.
Psychiatric comorbidity is frequent in rheumatoid arthritis (RA) and complicates treatment. The present study was undertaken to describe the impact of psychiatric comorbidity on health care use (utilization) in RA.
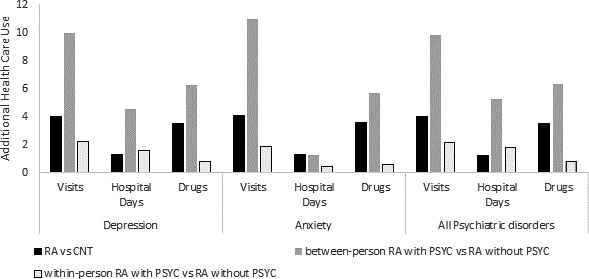
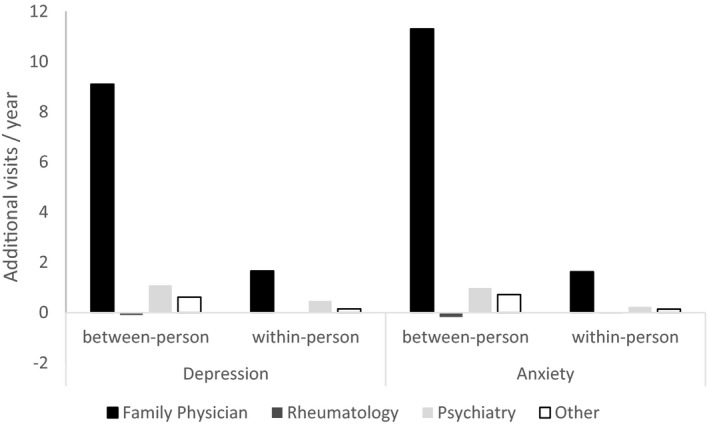
We accessed administrative health data (1984-2016) and identified a prevalent cohort with diagnosed RA. Cases of RA (n = 12,984) were matched for age, sex, and region of residence with 5 controls (CNT) per case (n = 64,510). Within each cohort, we identified psychiatric morbidities (depression, anxiety, bipolar disorder, and schizophrenia [PSYC]), with active PSYC defined as ≥2 visits per year. For the years 2006-2016, annual rates of ambulatory care visits (mean ± SD per person) categorized by provider (family physician [FP], rheumatologist, psychiatrist, other specialist), hospitalization (% of cohort), days of hospitalization (mean ± SD), and dispensed drug types (mean ± SD per person) were compared among 4 groups (CNT, CNT plus PSYC, RA, and RA plus PSYC) using generalized linear models adjusted for age, sex, rural versus urban residence, income quintile, and total comorbidities. Estimated rates are reported with 95% confidence intervals (95% CIs). We tested within-person and RA-PSYC interaction effects.
Subjects with RA were mainly female (72%) and urban residents (59%), with a mean ± SD age of 54 ± 16 years. Compared to RA without PSYC, RA with PSYC had more than additive (synergistic) visits (standardized mean difference [SMD] 10.92 [95% CI 10.25, 11.58]), hospitalizations (SMD 13% [95% CI 0.11, 0.14]), and hospital days (SMD 3.63 [95% CI 3.06, 4.19]) and were dispensed 6.85 more medication types (95% CI 6.43, 7.27). Cases of RA plus PSYC had increased visits to FPs (an additional SMD 8.92 [95% CI 8.35, 9.46] visits). PSYC increased utilization in within-person models.
Managing psychiatric comorbidity effectively may reduce utilization in RA.
精神共病在类风湿关节炎(RA)中很常见,且使治疗复杂化。本研究旨在描述精神共病对 RA 患者医疗保健利用(使用率)的影响。
我们访问了行政健康数据(1984-2016 年),并确定了一个患有诊断性 RA 的现患队列。将 RA 病例(n=12984)按年龄、性别和居住地区与每例病例的 5 名对照(CNT)相匹配(n=64510)。在每个队列中,我们确定了精神障碍(抑郁、焦虑、双相情感障碍和精神分裂症[PSYC]),每年≥2 次就诊定义为有精神障碍。在 2006-2016 年期间,根据提供者(家庭医生[FP]、风湿病专家、精神科医生、其他专科医生)对每年的门诊就诊次数(人均平均值±标准差)、住院率(队列的百分比)、住院天数(人均平均值±标准差)和配药类型(人均平均值±标准差)进行比较,采用广义线性模型进行调整,包括年龄、性别、农村与城市居住、收入五分位数和总合并症。报告的估计率带有 95%置信区间(95%CI)。我们测试了个体内和 RA-PSYC 相互作用效应。
RA 患者主要为女性(72%)和城市居民(59%),平均年龄为 54±16 岁。与无 PSYC 的 RA 相比,有 PSYC 的 RA 就诊次数(标准化均数差[SMD] 10.92[95%CI 10.25,11.58])、住院率(SMD 13%[95%CI 0.11,0.14])和住院天数(SMD 3.63[95%CI 3.06,4.19])都呈超相加(协同)趋势,配药类型也增加了 6.85 种(95%CI 6.43,7.27)。RA 加 PSYC 的病例就诊 FP 次数增加(额外的 SMD 8.92[95%CI 8.35,9.46]就诊)。PSYC 在个体内模型中增加了利用率。
有效管理精神共病可能会降低 RA 的利用率。