Caputo Damiano, Coppola Alessandro, Cascone Chiara, Angeletti Silvia, Ciccozzi Massimo, La Vaccara Vincenzo, Coppola Roberto
Department of Surgery, University Campus Bio-Medico of Rome, Rome, Italy.
Unit of Clinical Laboratory Science, University Campus Bio-Medico of Rome, Rome, Italy.
Ann Med Surg (Lond). 2020 Jul 15;57:56-61. doi: 10.1016/j.amsu.2020.07.018. eCollection 2020 Sep.
Postoperative day 1-drains amylase (POD1-DA) values are commonly used to predict the risk of pancreatic fistula (PF) after pancreaticoduodenectomy (PD). Perioperative inflammatory biomarkers have been associated to higher risk of complications in different oncological surgeries. Aim of this study was to investigate the utility of the combination of preoperative inflammatory biomarkers (PIBs) with POD1-DA levels in predicting grade C PF.
From a prospective collected database of 317 consecutive pancreaticoduodenectomies, data regarding POD1-DA levels and PIBs as neutrophil-to-lymphocyte ratio (NRL), derived neutrophil-to-lymphocyte ratio (dNRL), platelet-to-lymphocyte ratio (PLR) were analyzed in 227 cases. P-values <0.05 were considered statistically significant. Receiver operating characteristic (ROC) curves defined the optimal thresholds for biomarkers and drains amylase values and their accuracy to predict PF. Furthermore, the Positive Predictive Value (PPV) was computed to evaluate the probability to develop PF combining PIBs and drains amylase values. Combination of drains amylase and different PIBs cut-offs were used to evaluate the risk of grade C PF.
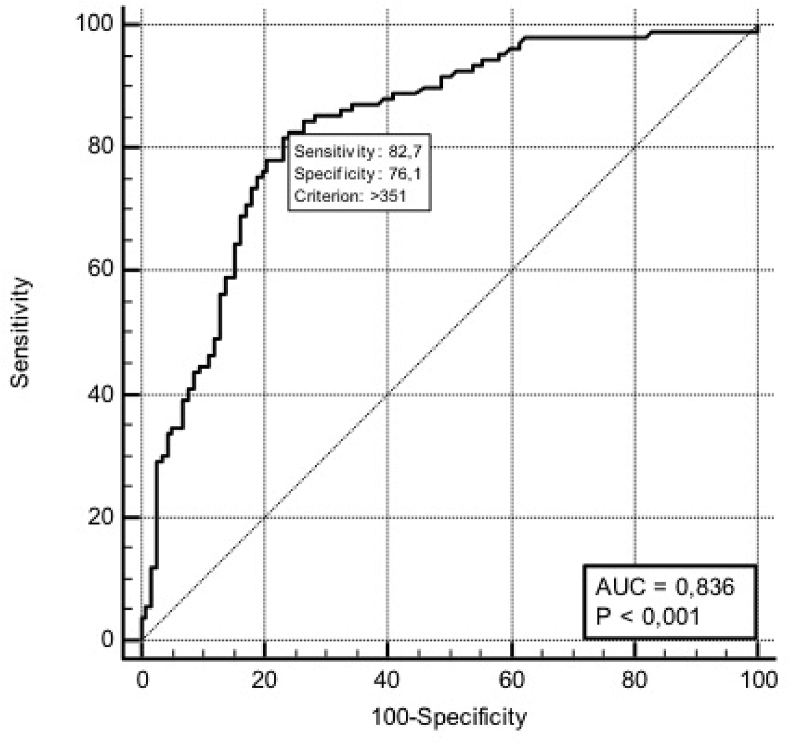
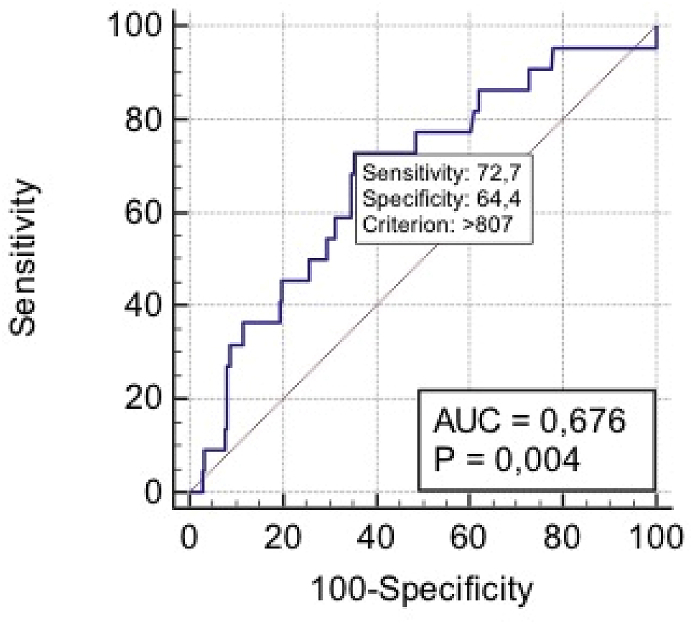
A POD1-DA level of 351 U/L significantly predicted PF (sensitivity 82.7%, specificity 76%, AUC 0.836; p < 0.001) with a PPV of 76.5% and a NPV of 82.6%.POD1-DA levels ≥807 U/L significantly predicted grade C PF (sensitivity 72.7%, specificity 64.4%, AUC 0.676; p = 0.004) with a PPV of 17.8% and a NPV of 95.6%.Notably, this last PPV increased from 17.8% to 89% when PIBs, at different cut-offs, were combined with POD1-DA at the value ≥ 807 U/L.
PIBs significantly improve POD1-DA ability in predicting grade C PF after PD.
术后第1天引流液淀粉酶(POD1 - DA)值常用于预测胰十二指肠切除术(PD)后胰瘘(PF)的风险。围手术期炎症生物标志物与不同肿瘤手术中较高的并发症风险相关。本研究的目的是探讨术前炎症生物标志物(PIBs)与POD1 - DA水平联合用于预测C级PF的效用。
从一个前瞻性收集的包含317例连续胰十二指肠切除术的数据库中,分析了227例患者的POD1 - DA水平以及作为中性粒细胞与淋巴细胞比值(NRL)、衍生中性粒细胞与淋巴细胞比值(dNRL)、血小板与淋巴细胞比值(PLR)的PIBs数据。P值<0.05被认为具有统计学意义。受试者工作特征(ROC)曲线确定了生物标志物和引流液淀粉酶值的最佳阈值及其预测PF的准确性。此外,计算阳性预测值(PPV)以评估结合PIBs和引流液淀粉酶值发生PF的概率。使用引流液淀粉酶和不同PIBs临界值的组合来评估C级PF的风险。
POD1 - DA水平为351 U/L可显著预测PF(敏感性82.7%,特异性76%,AUC 0.836;p < 0.001),PPV为76.5%,NPV为82.6%。POD1 - DA水平≥807 U/L可显著预测C级PF(敏感性72.7%,特异性64.4%,AUC 0.676;p = 0.004),PPV为17.8%,NPV为95.6%。值得注意的是,当不同临界值的PIBs与≥807 U/L的POD1 - DA值联合使用时,最后的PPV从17.8%增加到89%。
PIBs显著提高了POD1 - DA预测PD后C级PF的能力。