Division of Cardiology Kokura Memorial Hospital Kitakyushu Japan.
Department of Cardiology Keio University School of Medicine Tokyo Japan.
J Am Heart Assoc. 2020 Aug 4;9(15):e016952. doi: 10.1161/JAHA.120.016952. Epub 2020 Jul 28.
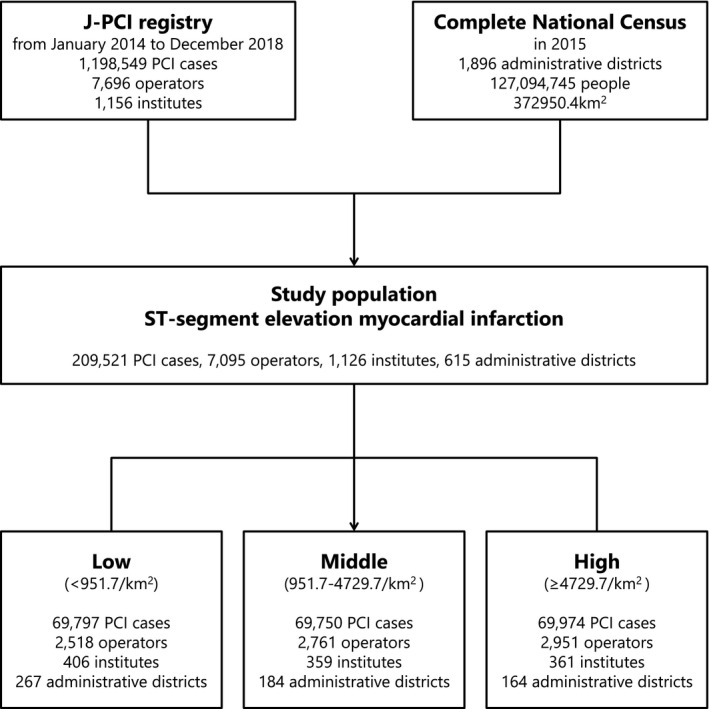
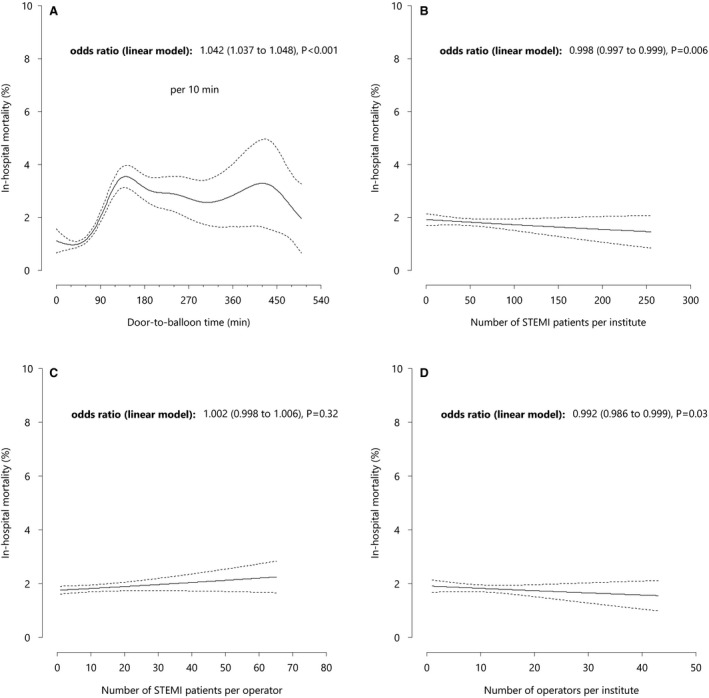
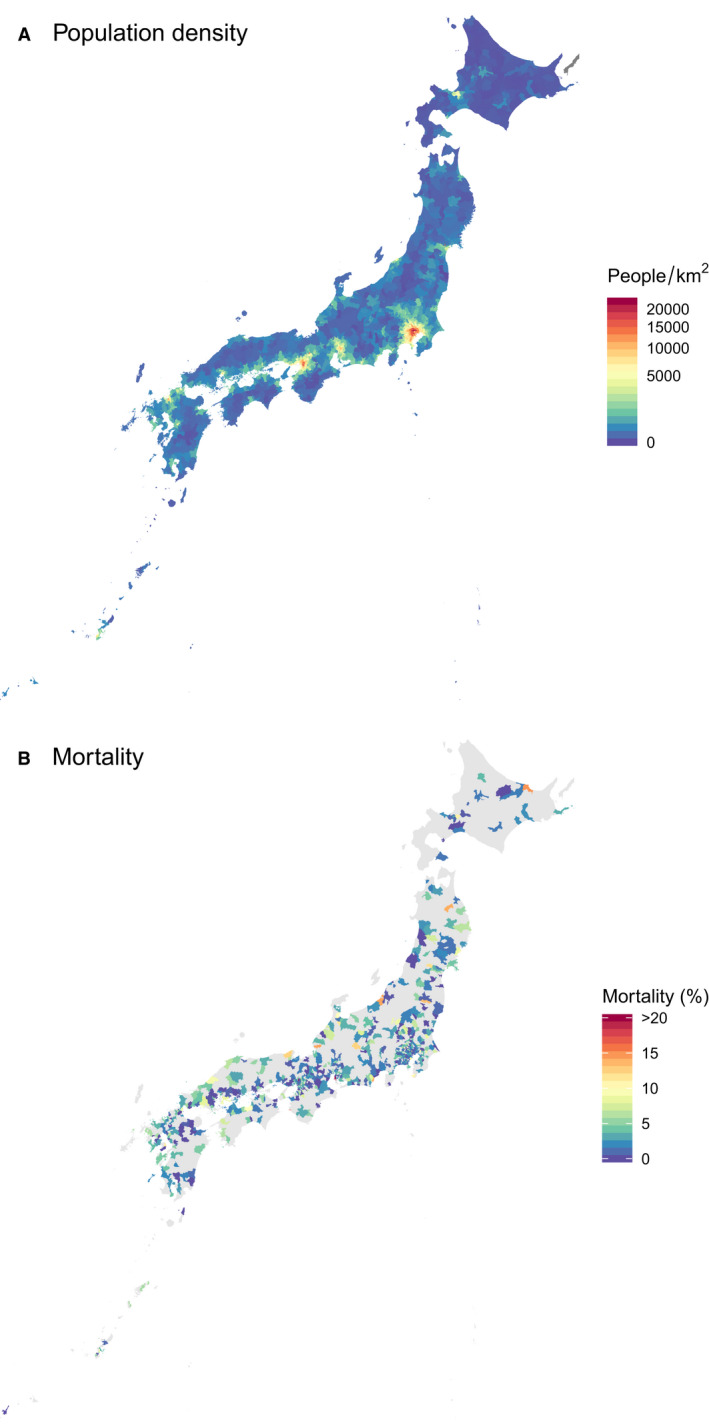
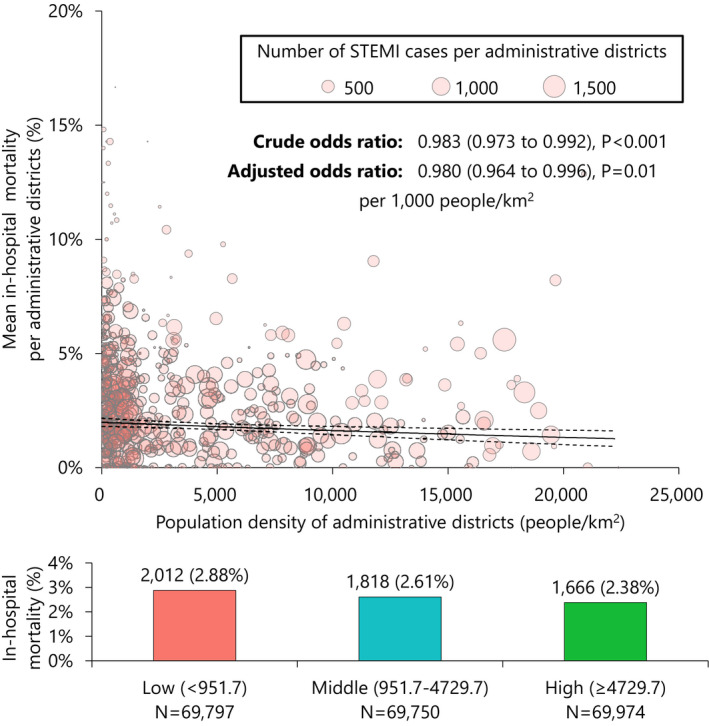
Background Despite recent progress in the treatment of ST-segment-elevation myocardial infarction, data on geographic disparities application of the evidence-based therapy remain limited. Methods and Results The J-PCI (Japanese Percutaneous Coronary Intervention) registry is a nationwide registry to assure the quality of delivered care. Between January 2014 and December 2018, 209 521 patients underwent percutaneous coronary intervention for ST-segment-elevation myocardial infarction in 1126 institutions. The patients were divided into tertiles according to the population density (PD) of the percutaneous coronary intervention institution location (low: <951.7/km, n = 69 797; medium: 951.7-4729.7/km, n = 69 750; high: ≥4729.7/km, n = 69 974). Patients treated in high PD administrative districts were younger and more likely to be male. No significant correlation was observed between PD and door-to-balloon time (regression coefficients: 0.036 per 1000 people/km; 95% CI, -0.232 to 0.304; = 0.79). Patients treated in low-PD areas had higher crude in-hospital mortality rates than those treated in high-PD areas (low: 2.89%; medium: 2.60%; high: 2.38%; < 0.001); PD and in-hospital mortality had a significantly inverse association, before and after adjusting for baseline characteristics (crude odds ratio [OR], 0.983 per 1000/km; 95% CI, 0.973-0.992; < 0.001; adjusted OR, 0.980 per 1000/km; 95% CI, 0.964-0.996; = 0.01, respectively). Higher-PD districts had more operators per institution (low: 6; interquartile range, 3-10; medium: 7; IQR, 3-13; high: 8; IQR, 5-13; < 0.001), suggesting an inverse association with in-hospital mortality (OR, 0.992; 95% CI, 0.986-0.999; = 0.03). Conclusions Geographic inequality was observed in in-hospital mortality of patients with ST-segment-elevation myocardial infarction who underwent percutaneous coronary intervention. Variation in the number of operators per institution, rather than traditional quality indicators (eg, door-to-balloon time) might explain the difference in in-hospital mortality.
尽管 ST 段抬高型心肌梗死的治疗取得了近期进展,但有关证据为基础的治疗方法在地理差异方面的应用的数据仍有限。
J-PCI(日本经皮冠状动脉介入治疗)注册研究是一项旨在确保提供的治疗质量的全国性注册研究。2014 年 1 月至 2018 年 12 月,1126 家医疗机构对 209521 例 ST 段抬高型心肌梗死患者进行了经皮冠状动脉介入治疗。根据经皮冠状动脉介入治疗机构所在地的人口密度(PD),将患者分为 3 个三分位组(低:<951.7/km,n=69797;中:951.7-4729.7/km,n=69750;高:≥4729.7/km,n=69974)。在高 PD 行政区域接受治疗的患者年龄较小,且更可能为男性。PD 与门球时间之间无明显相关性(回归系数:每 1000 人/km 增加 0.036;95%CI,-0.232 至 0.304;=0.79)。与高 PD 地区相比,低 PD 地区患者的住院死亡率更高(低:2.89%;中:2.60%;高:2.38%;<0.001);PD 和住院死亡率之间存在显著的负相关,在调整基线特征前后均如此(未经调整的优势比[OR],每 1000/km 降低 0.983;95%CI,0.973-0.992;<0.001;调整后的 OR,每 1000/km 降低 0.980;95%CI,0.964-0.996;=0.01)。PD 较高的地区每个机构的操作人员数量更多(低:6;四分位间距,3-10;中:7;IQR,3-13;高:8;IQR,5-13;<0.001),这表明与住院死亡率呈负相关(OR,0.992;95%CI,0.986-0.999;=0.03)。
ST 段抬高型心肌梗死患者经皮冠状动脉介入治疗后,其住院死亡率存在地理差异。每个机构的操作人员数量的差异(而非传统的质量指标,如门球时间)可能解释了住院死亡率的差异。