Piera-Jiménez Jordi, Winters Marjolein, Broers Eva, Valero-Bover Damià, Habibovic Mirela, Widdershoven Jos W M G, Folkvord Frans, Lupiáñez-Villanueva Francisco
Open Evidence Research Group, Universitat Oberta de Catalunya, Barcelona, Spain.
Department of R&D, Badalona Serveis Assistencials, Badalona, Spain.
J Med Internet Res. 2020 Jul 28;22(7):e17351. doi: 10.2196/17351.
During the last few decades, preventing the development of cardiovascular disease has become a mainstay for reducing cardiovascular morbidity and mortality. It has been suggested that interventions should focus more on committed approaches of self-care, such as electronic health techniques.
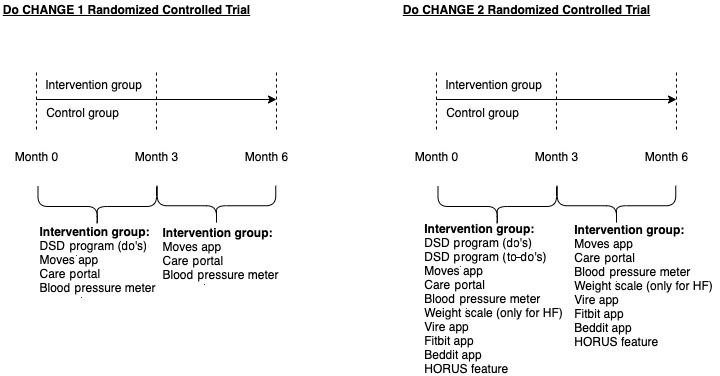
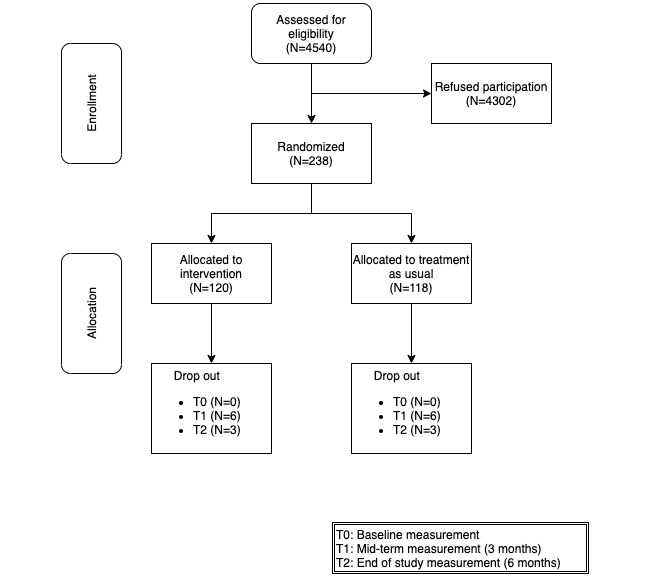
This study aimed to provide evidence to understand the financial consequences of implementing the "Do Cardiac Health: Advanced New Generation Ecosystem" (Do CHANGE 2) intervention, which was evaluated in a multisite randomized controlled trial to change the health behavior of patients with cardiovascular disease.
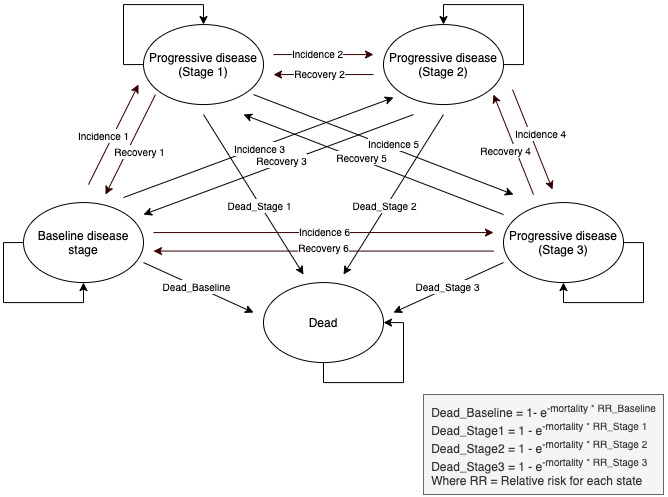
The cost-effectiveness analysis of the Do CHANGE 2 intervention was performed with the Monitoring and Assessment Framework for the European Innovation Partnership on Active and Healthy Ageing tool, based on a Markov model of five health states. The following two types of costs were considered for both study groups: (1) health care costs (ie, costs associated with the time spent by health care professionals on service provision, including consultations, and associated unplanned hospitalizations, etc) and (2) societal costs (ie, costs attributed to the time spent by patients and informal caregivers on care activities).
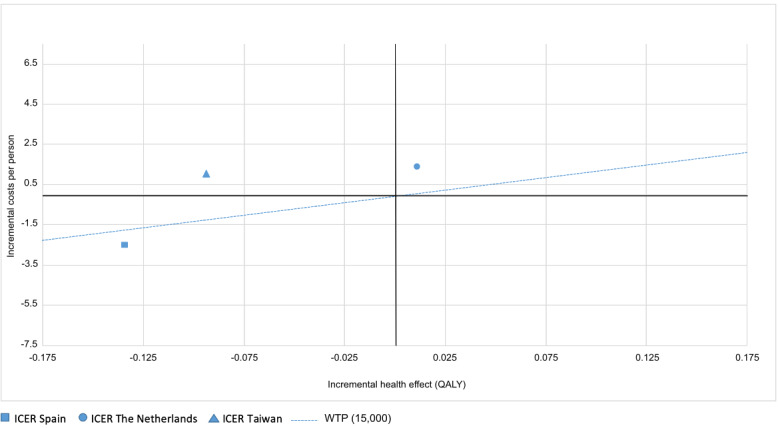
The Do CHANGE 2 intervention was less costly in Spain (incremental cost was -€2514.90) and more costly in the Netherlands and Taiwan (incremental costs were €1373.59 and €1062.54, respectively). Compared with treatment as usual, the effectiveness of the Do CHANGE 2 program in terms of an increase in quality-adjusted life-year gains was slightly higher in the Netherlands and lower in Spain and Taiwan.
In general, we found that the incremental cost-effectiveness ratio strongly varied depending on the country where the intervention was applied. The Do CHANGE 2 intervention showed a positive cost-effectiveness ratio only when implemented in Spain, indicating that it saved financial costs in relation to the effect of the intervention.
ClinicalTrials.gov NCT03178305; https://clinicaltrials.gov/ct2/show/NCT03178305.
在过去几十年中,预防心血管疾病的发展已成为降低心血管发病率和死亡率的主要手段。有人建议干预措施应更多地侧重于自我护理的既定方法,如电子健康技术。
本研究旨在提供证据,以了解实施“关爱心脏健康:新一代先进生态系统”(Do CHANGE 2)干预措施的财务后果,该干预措施在一项多中心随机对照试验中进行了评估,以改变心血管疾病患者的健康行为。
基于五个健康状态的马尔可夫模型,使用欧洲积极健康老龄化创新伙伴关系监测与评估框架工具对Do CHANGE 2干预措施进行成本效益分析。两个研究组均考虑以下两类成本:(1)医疗保健成本(即与医护人员提供服务所花费时间相关的成本,包括咨询以及相关的非计划住院等)和(2)社会成本(即患者和非正式护理人员在护理活动上花费时间所产生的成本)。
Do CHANGE 2干预措施在西班牙成本较低(增量成本为-2514.90欧元),在荷兰和台湾成本较高(增量成本分别为1373.59欧元和1062.54欧元)。与常规治疗相比,Do CHANGE 2计划在质量调整生命年增益增加方面的效果在荷兰略高,在西班牙和台湾较低。
总体而言我们发现,增量成本效益比因干预措施实施的国家不同而有很大差异。Do CHANGE 2干预措施仅在西班牙实施时显示出正的成本效益比,表明相对于干预效果而言它节省了财务成本。
ClinicalTrials.gov NCT0******;https://clinicaltrials.gov/ct2/show/NCT0******。 (注:原文中NCT编号部分数字未完整给出,翻译时保留原文格式)