Yoshiaki Tanno Fabio, Srougi Victor, Almeida Madson Q, Ide Yamauchi Fernando, Morbeck Almeida Coelho Fernando, Nishi Mirian Yumie, Claudia Nogueira Zerbini Maria, Silvia Correa Soares Iracy, Adelaide Albergaria Pereira Maria, Laiz Silva Charchar Helaine, Meneses Ferreira Lacombe Amanda, Balderrama Brondani Vania, Srougi Miguel, Carlos Nahas Willian, Mendonca Berenice B, Luis Chambô José, Candida Barisson Villares Fragoso Maria
Divisão de Urologia, Hospital das Clínicas, Faculdade de Medicina da Universidade de São Paulo, São Paulo, Brazil.
Unidade de Suprarrenal, Laboratório de Hormônios e Genética Molecular LIM/42, Serviço de Endocrinologia e Metabologia, Hospital das Clínicas, Faculdade de Medicina da Universidade de São Paulo, São Paulo, Brazil.
J Endocr Soc. 2020 Jul 22;4(8):bvaa083. doi: 10.1210/jendso/bvaa083. eCollection 2020 Aug 1.
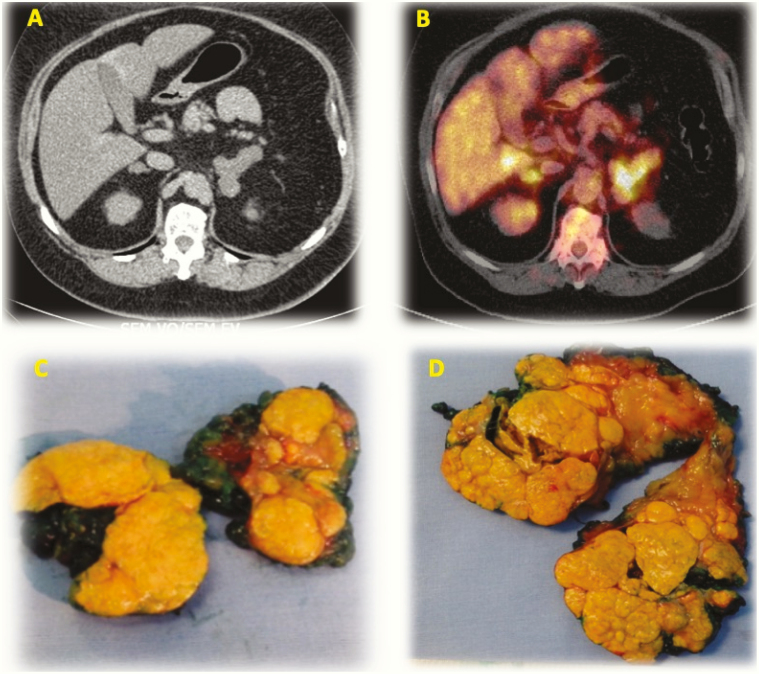
This prospective study presents the results of a new approach in the treatment of primary macronodular adrenal hyperplasia (PMAH), with simultaneous total adrenalectomy of the larger adrenal gland and partial adrenalectomy of the contralateral adrenal gland (adrenal-sparing surgery).
We performed a prospective study including 17 patients with PMAH treated surgically with adrenal-sparing surgery in a tertiary referral hospital, with a median follow-up of 41 months. Clinical, hormonal, and genetic parameters were evaluated before surgery and during follow-up. All patients had at least 1 radiological examination before and after the procedure.
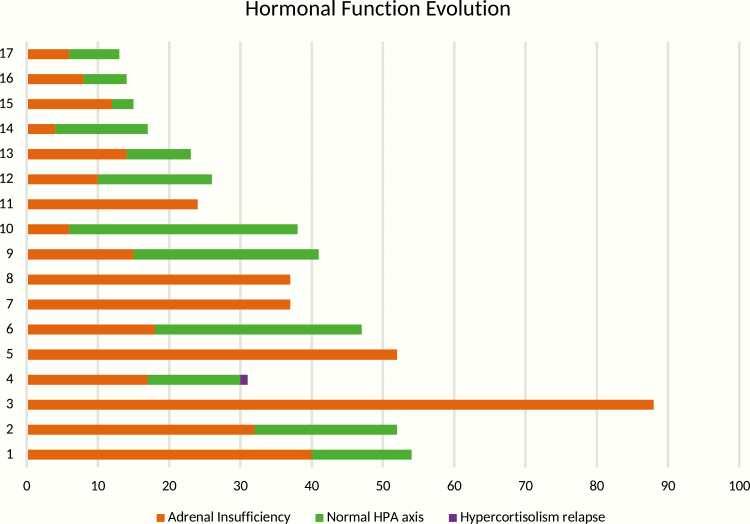
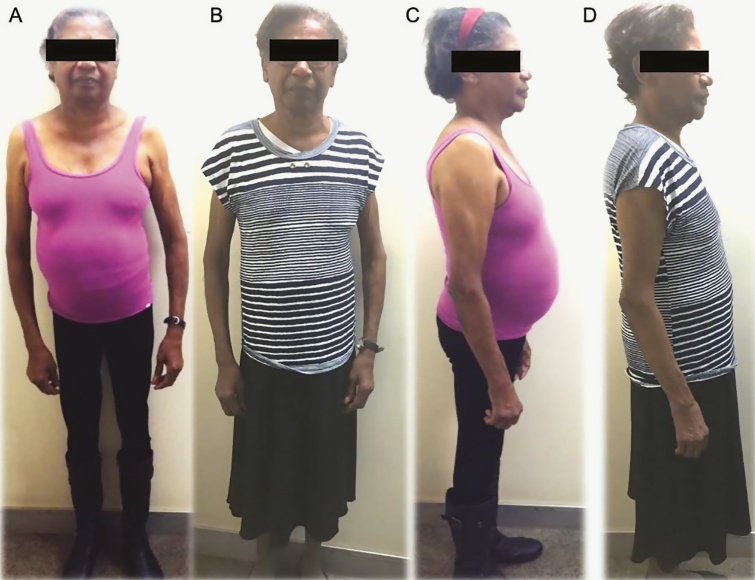
Among the 17 patients, all but 1 patient had complete hypercortisolism control, and 12 recovered normal adrenal function after surgery. Significant improvement in clinical parameters was observed: weight loss ( = .004); reduction of both systolic ( = .001) and diastolic ( = .001) blood pressure; and reduction in the number of antihypertensive drugs ( < .001). Intra-, peri-, and postoperative complications were not observed.
Adrenal-sparing surgery is a safe and feasible procedure to treat patients with PMAH, providing a substantial chance of hypercortisolism control without the disadvantages of lifetime corticosteroid replacement.
本前瞻性研究展示了一种治疗原发性大结节性肾上腺增生(PMAH)的新方法,即对较大的肾上腺进行同期全肾上腺切除术,并对侧肾上腺进行部分肾上腺切除术(保留肾上腺手术)。
我们进行了一项前瞻性研究,纳入了17例在三级转诊医院接受保留肾上腺手术治疗的PMAH患者,中位随访时间为41个月。在手术前和随访期间评估临床、激素和基因参数。所有患者在手术前后至少进行了1次影像学检查。
17例患者中,除1例患者外,其余所有患者的皮质醇增多症均得到完全控制,12例患者术后肾上腺功能恢复正常。观察到临床参数有显著改善:体重减轻(P = .004);收缩压(P = .001)和舒张压(P = .001)均降低;降压药物数量减少(P < .001)。未观察到术中、围手术期和术后并发症。
保留肾上腺手术是治疗PMAH患者的一种安全可行的方法,在不具有终身皮质类固醇替代治疗缺点的情况下,有很大机会控制皮质醇增多症。