Department of Surgery, Division of Trauma and Critical Care, Jackson Memorial Hospital Ryder Trauma Center, University of Miami, Miami, FL, USA.
Department of Surgery, Division of Trauma and Critical Care Surgery, Keck School of Medicine, LAC+USC Medical Center, University of Southern California, 2051 Marengo Street, Inpatient Tower, C5L100, Los Angeles, CA, 90033, USA.
World J Surg. 2020 Nov;44(11):3743-3750. doi: 10.1007/s00268-020-05712-x. Epub 2020 Jul 30.
Hypocalcemia is cited as a complication of massive transfusion. However, this is not well studied as a primary outcome in trauma patients. Our primary outcome was to determine if transfusion of packed red blood cells (pRBC) was an independent predictor of severe hypocalcemia (ionized calcium ≤ 3.6 mg/dL).
Retrospective, single-center study (01/2004-12/2014) including all trauma patients ≥ 18 yo presenting to the ED with an ionized calcium (iCa) level drawn. Variables extracted included demographics, interventions, outcomes, and iCa. Regression models identified independent risk factors for severe hypocalcemia (SH).
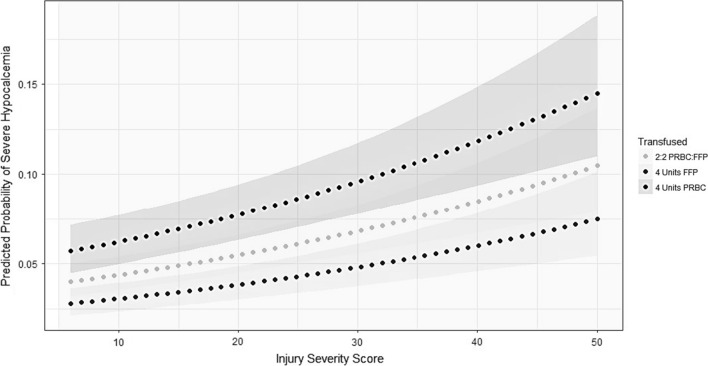
Seven thousand four hundred and thirty-one included subjects, 716 (9.8%) developed SH within 48 h of admission. Median age: 39 (Range: 18-102), systolic blood pressure: 131 (IQR: 114-150), median Glasgow Coma Scale (GCS): 15 (IQR: 10-15), Injury Severity Score (ISS): 14 (IQR: 9-24). SH patients were more likely to have depressed GCS (13 vs 15, p < 0.0001), hypotension (23.2% vs 5.1%, p < 0.0001) and tachycardia (57.0% vs 41.9%, p < 0.0001) compared to non-SH patients. They also had higher emergency operative rate (71.8% vs 29%, p < 0.0001) and higher blood administration prior to minimum iCa [pRBC: (8 vs 0, p < 0.0001), FFP: (4 vs 0, p < 0.0001), platelet: (1 vs 0, p < 0.0001)]. Multivariable analysis revealed penetrating mechanism (AOR: 1.706), increased ISS (AOR: 1.029), and higher pRBC (AOR: 1.343) or FFP administered (AOR: 1.097) were independent predictors of SH. SH was an independent predictor of mortality (AOR: 2.658). Regression analysis identified a significantly higher risk of SH at pRBC + FFP administration of 4 units (AOR: 18.706, AUC:. 897 (0.884-0.909).
Transfusion of pRBC is an independent predictor of SH and is associated with increased mortality. The predicted probability of SH increases as pRBC + FFP administration increases.
低钙血症被认为是大量输血的并发症。然而,在创伤患者中,这并不是一个作为主要结果的研究。我们的主要结果是确定输注浓缩红细胞(pRBC)是否是严重低钙血症(离子钙 ≤ 3.6mg/dL)的独立预测因子。
回顾性、单中心研究(2004 年 1 月至 2014 年 12 月),纳入所有年龄≥18 岁的创伤患者,在急诊科抽取离子钙(iCa)水平。提取的变量包括人口统计学、干预措施、结局和 iCa。回归模型确定严重低钙血症(SH)的独立危险因素。
7431 例纳入研究的患者中,716 例(9.8%)在入院后 48 小时内出现 SH。中位数年龄为 39 岁(范围:18-102),收缩压为 131mmHg(IQR:114-150),格拉斯哥昏迷评分(GCS)中位数为 15 分(IQR:10-15),损伤严重程度评分(ISS)中位数为 14 分(IQR:9-24)。SH 患者的 GCS 评分更可能降低(13 分比 15 分,p<0.0001)、低血压(23.2%比 5.1%,p<0.0001)和心动过速(57.0%比 41.9%,p<0.0001),而非 SH 患者。他们的急诊手术率也更高(71.8%比 29%,p<0.0001),在最低 iCa 之前接受的血液制品输注量也更高[浓缩红细胞:(8 单位比 0 单位,p<0.0001),FFP:(4 单位比 0 单位,p<0.0001),血小板:(1 单位比 0 单位,p<0.0001)]。多变量分析显示,穿透性机制(OR:1.706)、ISS 增加(OR:1.029),以及更高的浓缩红细胞(OR:1.343)或 FFP 输注(OR:1.097)是 SH 的独立预测因子。SH 是死亡率的独立预测因子(OR:2.658)。回归分析确定,在输注 4 单位浓缩红细胞+FFP 时,SH 的风险显著增加(OR:18.706,AUC:0.897(0.884-0.909)。
输注浓缩红细胞是 SH 的独立预测因子,并与死亡率增加相关。随着浓缩红细胞+FFP 的输注量增加,SH 的预测概率增加。