Clinical Neurosciences, Clinical and Experimental Sciences, Faculty of Medicine, University of Southampton, Southampton, UK.
Memory Assessment and Research Centre, Moorgreen Hospital, Southern Health NHS Foundation Trust, Southampton, UK.
Transl Psychiatry. 2020 Aug 3;10(1):267. doi: 10.1038/s41398-020-00954-8.
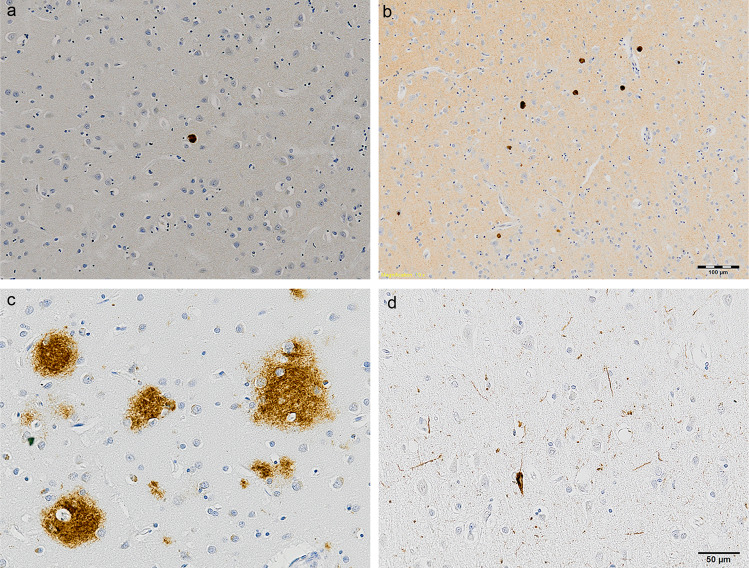
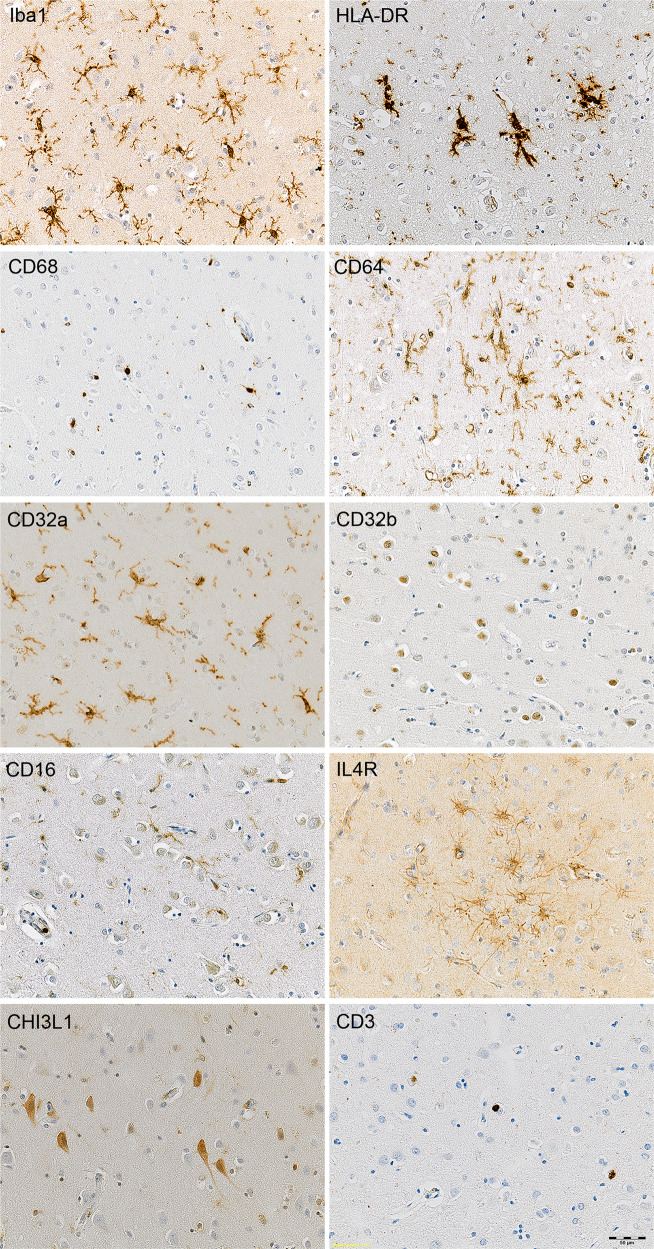
Dementia with Lewy bodies (DLB) is the second most common neurodegenerative cause of dementia, behind Alzheimer's disease (AD). It is now established that cerebral inflammation has a key role in the aetiology and progression of AD, but this has yet to be confirmed in DLB. We aimed to determine the neuroinflammatory profile in the cerebral cortex of a large cohort of DLB cases. Thirty post-mortem confirmed DLB cases and twenty-nine matched controls were immunolabelled (Brodmann area 21) and quantified for: neuropathology-αSYN, Aβ, P-tau; microglial phenotype-Iba1, HLA-DR, CD68, FcƴR (CD64, CD32a, CD32b, CD16); presence of T lymphocytes-CD3; and anti-inflammatory markers-IL4R, CHI3L1. Status spongiosis, as a marker of neuropil degeneration, was quantified using Haematoxylin and Eosin staining. We found no significant difference between groups in protein load for Iba1, HLA-DR, CD68, CD64, CD32b, IL4R, or CHI3L1, despite increased neuropathology in DLB. CD32a load was significantly lower, and CD16 load higher, in DLB compared with controls. There was no difference in status spongiosis between groups. Significantly more DLB cases than controls showed T-lymphocyte recruitment. Overall, we conclude that microglial activation is not a prominent feature of DLB, and that this may be associated with the relatively modest neuropil degeneration observed in DLB. Our findings, based on the largest post-mortem cohort to date exploring neuroinflammation in DLB, demonstrate a dissociation between protein deposition, neurodegeneration and microglial activation. The relative preservation of cortical structures in DLB suggests the dementia could be more amenable to potential therapies.
路易体痴呆(DLB)是仅次于阿尔茨海默病(AD)的第二大常见痴呆病因。目前已经确定,大脑炎症在 AD 的发病机制和进展中起关键作用,但尚未在 DLB 中得到证实。我们的目的是确定大量 DLB 病例大脑皮层的神经炎症特征。对 30 例经尸检证实的 DLB 病例和 29 例匹配对照进行免疫标记(Brodmann 区 21)和定量分析:神经病理学-αSYN、Aβ、P-tau;小胶质细胞表型-Iba1、HLA-DR、CD68、FcγR(CD64、CD32a、CD32b、CD16);T 淋巴细胞-CD3 的存在;以及抗炎标志物-IL4R、CHI3L1。使用苏木精和伊红染色定量评估作为神经原纤维退化标志物的海绵状变性状态。我们发现,尽管 DLB 患者的神经病理学表现增加,但 Iba1、HLA-DR、CD68、CD64、CD32b、IL4R 或 CHI3L1 的蛋白负荷在两组之间没有显著差异。与对照组相比,DLB 中 CD32a 的负荷显著降低,而 CD16 的负荷则升高。两组之间的海绵状变性状态没有差异。与对照组相比,DLB 病例中有更多的 T 淋巴细胞募集。总的来说,我们得出的结论是,小胶质细胞激活不是 DLB 的一个显著特征,这可能与 DLB 中观察到的相对较轻的神经原纤维退化有关。我们的发现基于迄今为止对 DLB 中神经炎症进行探索的最大尸检队列,表明蛋白沉积、神经退行性变和小胶质细胞激活之间存在分离。DLB 中皮质结构的相对保留表明,痴呆症可能更容易受到潜在治疗的影响。