Division of Cardiology Department of Pediatrics University of Toronto The Hospital for Sick Children Toronto Ontario Canada.
Boston Children's Hospital Harvard Medical School Boston MA.
J Am Heart Assoc. 2020 Aug 4;9(15):e016440. doi: 10.1161/JAHA.119.016440. Epub 2020 Jul 28.
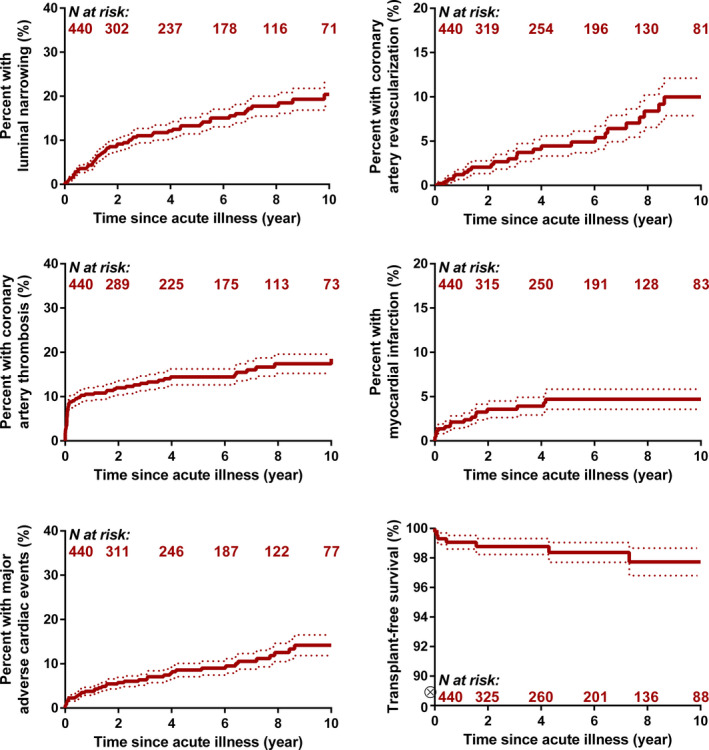
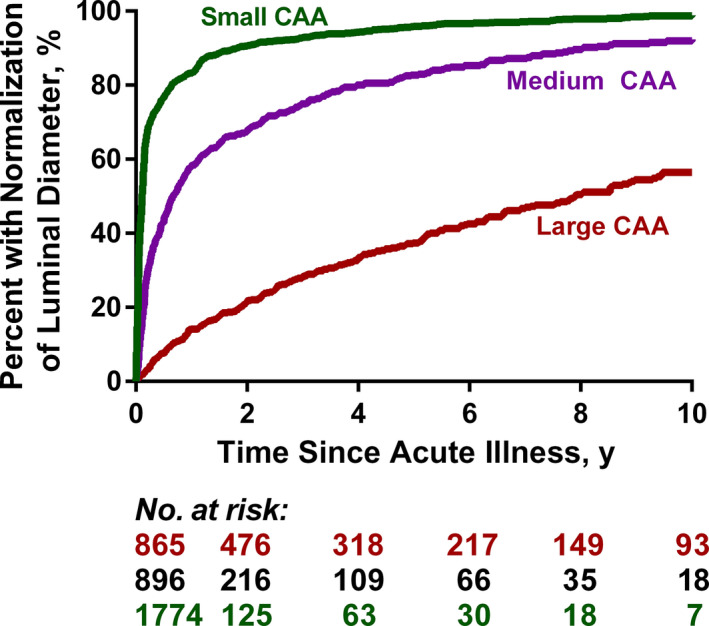
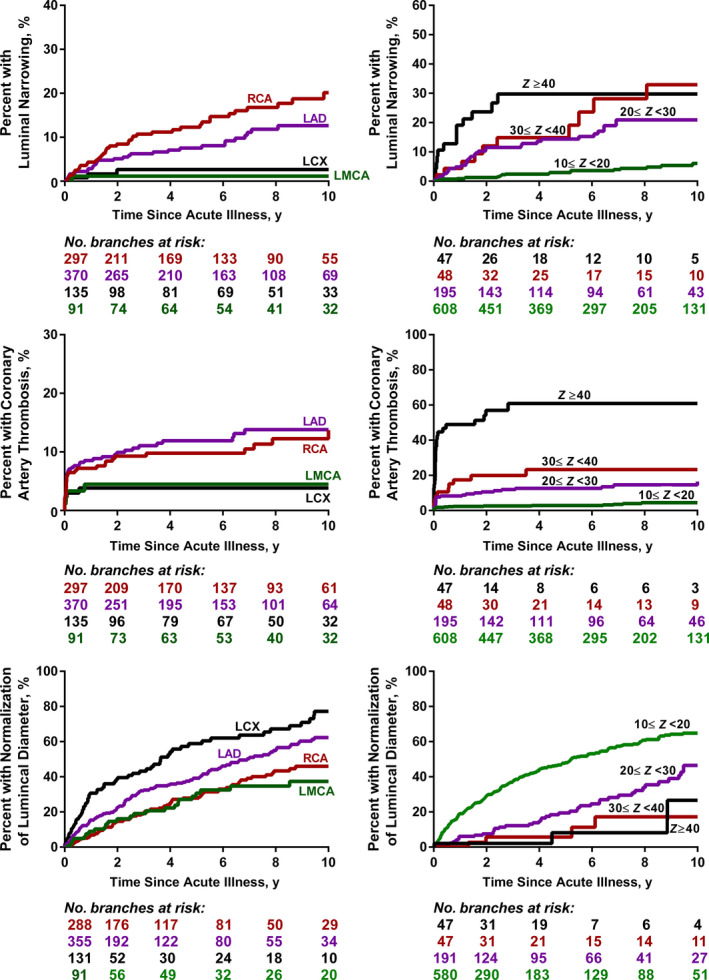
Background Coronary artery aneurysms (CAAs) may occur after Kawasaki disease (KD) and lead to important morbidity and mortality. As CAA in patients with KD are rare and heterogeneous lesions, prognostication and risk stratification are difficult. We sought to derive the cumulative risk and associated factors for cardiovascular complications in patients with CAAs after KD. Methods and Results A 34-institution international registry of 1651 patients with KD who had CAAs (maximum CAA score ≥2.5) was used. Time-to-event analyses were performed using the Kaplan-Meier method and Cox proportional hazard models for risk factor analysis. In patients with CAA scores ≥10, the cumulative incidence of luminal narrowing (>50% of lumen diameter), coronary artery thrombosis, and composite major adverse cardiovascular complications at 10 years was 20±3%, 18±2%, and 14±2%, respectively. No complications were observed in patients with a CAA score <10. Higher CAA score and a greater number of coronary artery branches affected were associated with increased risk of all types of complications. At 10 years, normalization of luminal diameter was noted in 99±4% of patients with small (2.5≤<5.0), 92±1% with medium (5.0≤<10), and 57±3% with large CAAs (≥10). CAAs in the left anterior descending and circumflex coronary artery branches were more likely to normalize. Risk factor analysis of coronary artery branch level outcomes was performed with a total of 893 affected branches with score ≥10 in 440 patients. In multivariable regression models, hazards of luminal narrowing and thrombosis were higher for patients with CAAs of the right coronary artery and left anterior descending branches, those with CAAs that had complex architecture (other than isolated aneurysms), and those with CAAs with scores ≥20. Conclusions For patients with CAA after KD, medium-term risk of complications is confined to those with maximum CAA scores ≥10. Further risk stratification and close follow-up, including advanced imaging, in patients with large CAAs is warranted.
川崎病(KD)后可发生冠状动脉瘤(CAA),并导致重要的发病率和死亡率。由于 KD 患者的 CAA 是罕见且异质性的病变,因此预后和风险分层较为困难。我们旨在探讨 KD 后 CAA 患者发生心血管并发症的累积风险及相关因素。
我们使用了一个由 1651 例 KD 合并 CAA(最大 CAA 评分≥2.5)患者组成的 34 家机构国际注册中心,采用 Kaplan-Meier 方法进行时间事件分析,并采用 Cox 比例风险模型进行危险因素分析。在 CAA 评分≥10 的患者中,10 年内管腔狭窄(管腔直径缩小>50%)、冠状动脉血栓形成和复合主要不良心血管并发症的累积发生率分别为 20±3%、18±2%和 14±2%。CAA 评分<10 的患者未观察到任何并发症。较高的 CAA 评分和受影响的冠状动脉分支数量与所有类型并发症的风险增加相关。10 年后,小(2.5< <5.0)、中(5.0< <10)和大(≥10)CAA 的患者管腔直径正常率分别为 99±4%、92±1%和 57±3%。左前降支和回旋支 CAA 更有可能恢复正常。对 440 例患者中 893 个 CAA 分支(共 440 例患者,评分≥10)进行了冠状动脉分支水平结局的危险因素分析。多变量回归模型显示,右冠状动脉和前降支 CAA、结构复杂(非孤立性动脉瘤)的 CAA 以及评分≥20 的 CAA 的患者,管腔狭窄和血栓形成的风险更高。
KD 后 CAA 患者的中期并发症风险仅限于最大 CAA 评分≥10 的患者。对于大 CAA 患者,需要进一步进行风险分层和密切随访,包括高级影像学检查。