Juravinski Cancer Centre, McMaster University, Hamilton, Canada.
Division of Hematology, Mayo Clinic Cancer Center, Jacksonville, FL, USA.
Leuk Lymphoma. 2020 Dec;61(13):3188-3197. doi: 10.1080/10428194.2020.1795159. Epub 2020 Aug 6.
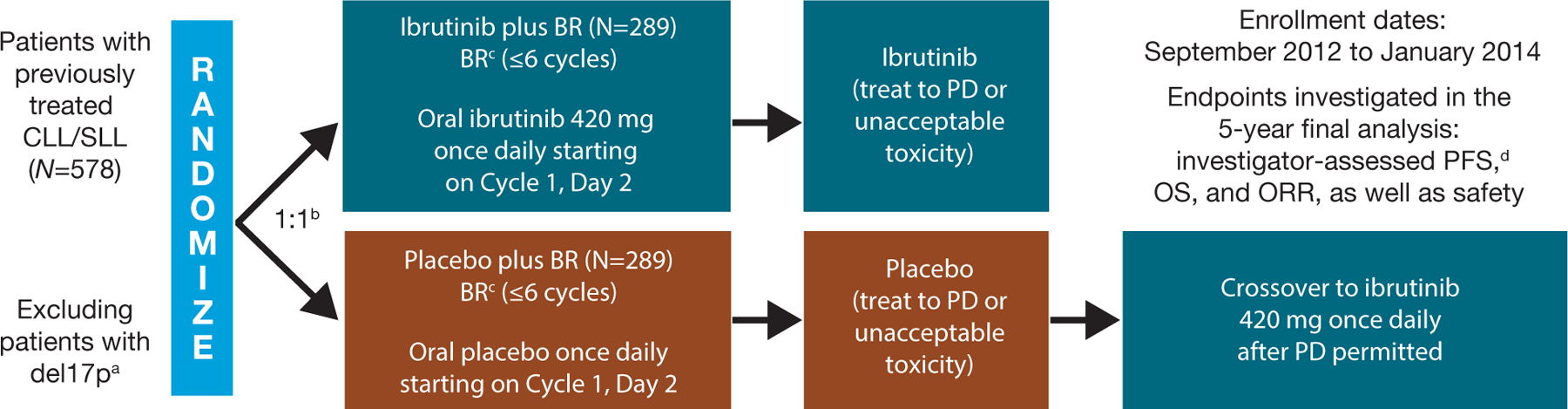
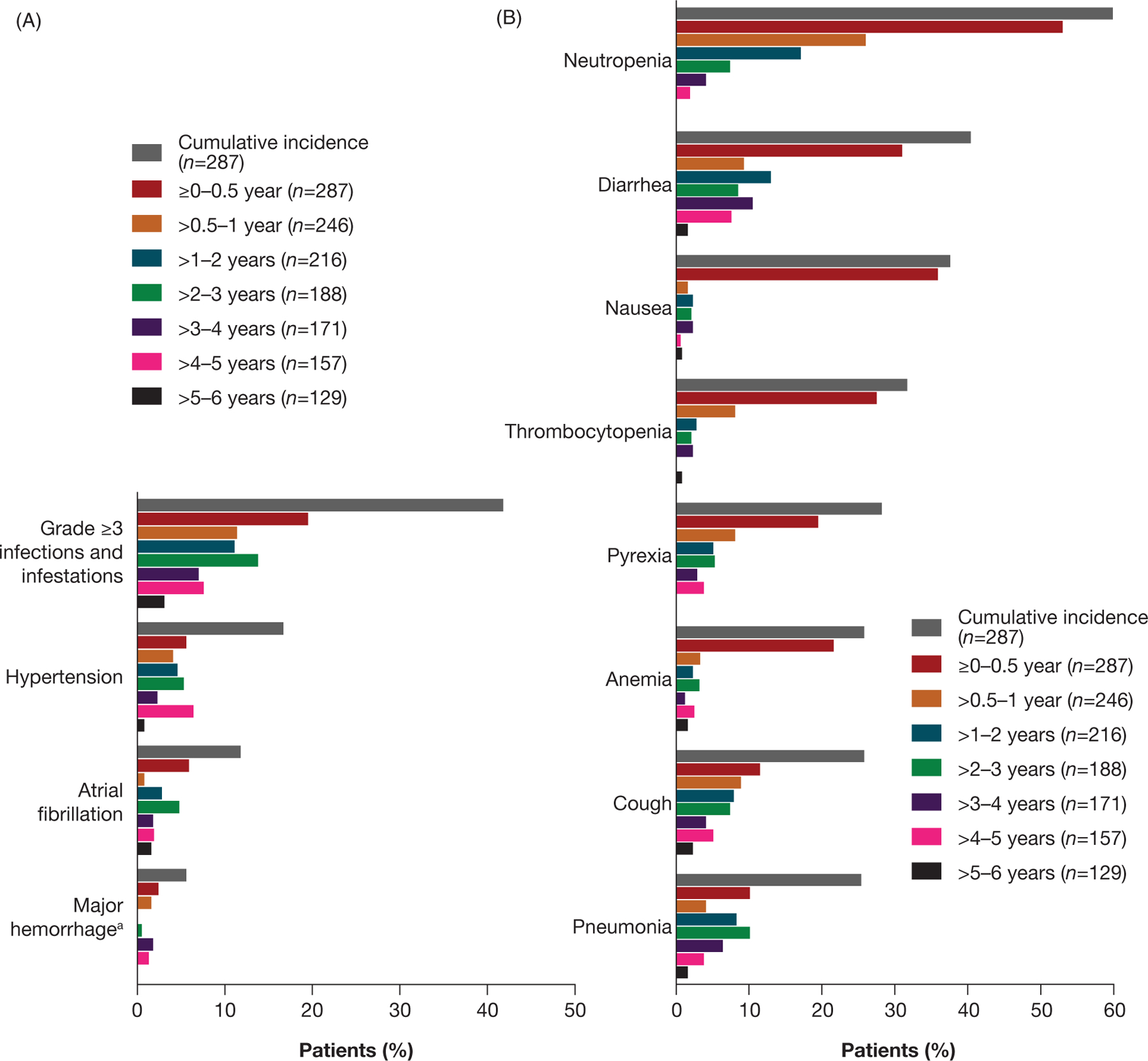
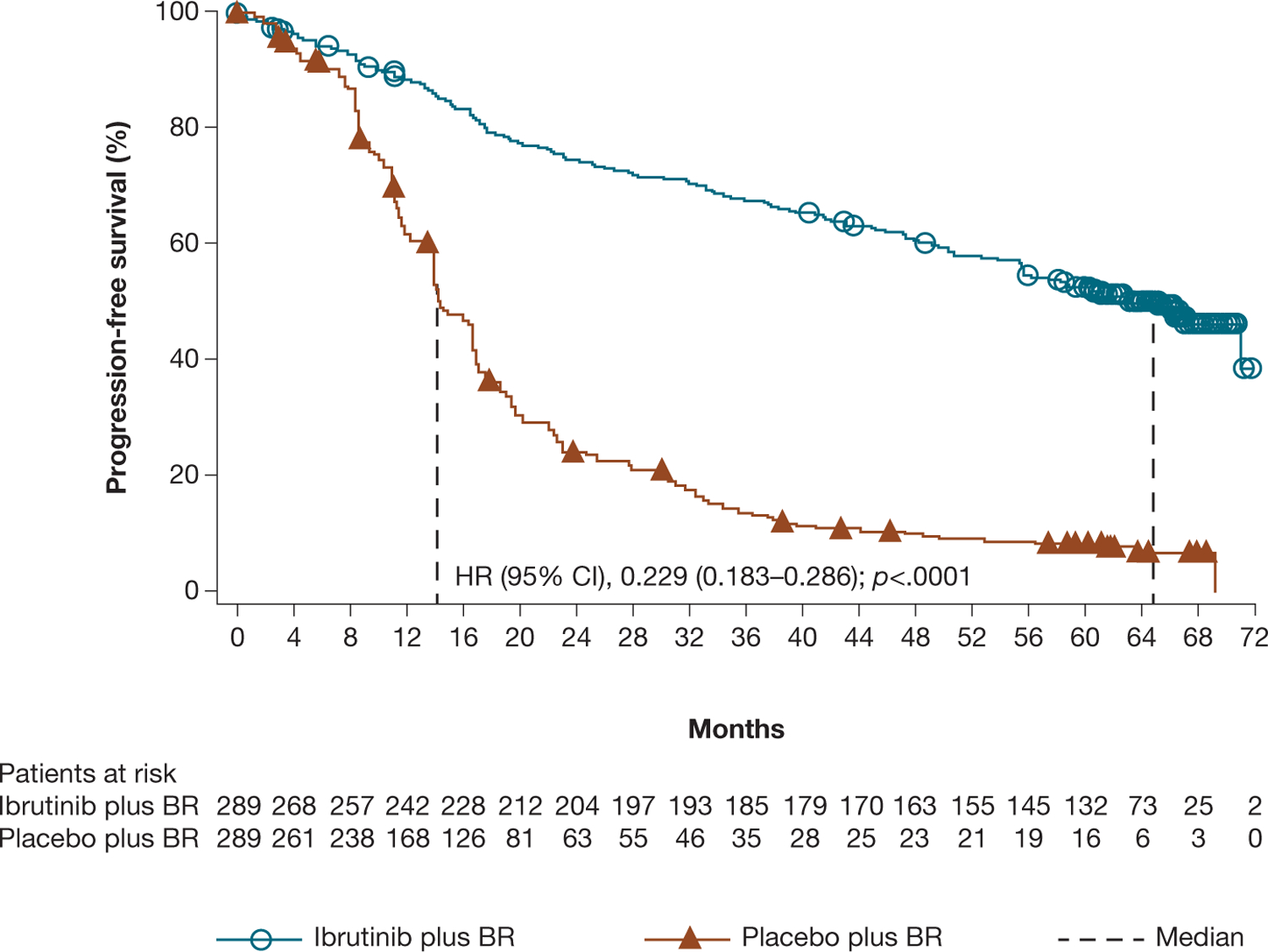
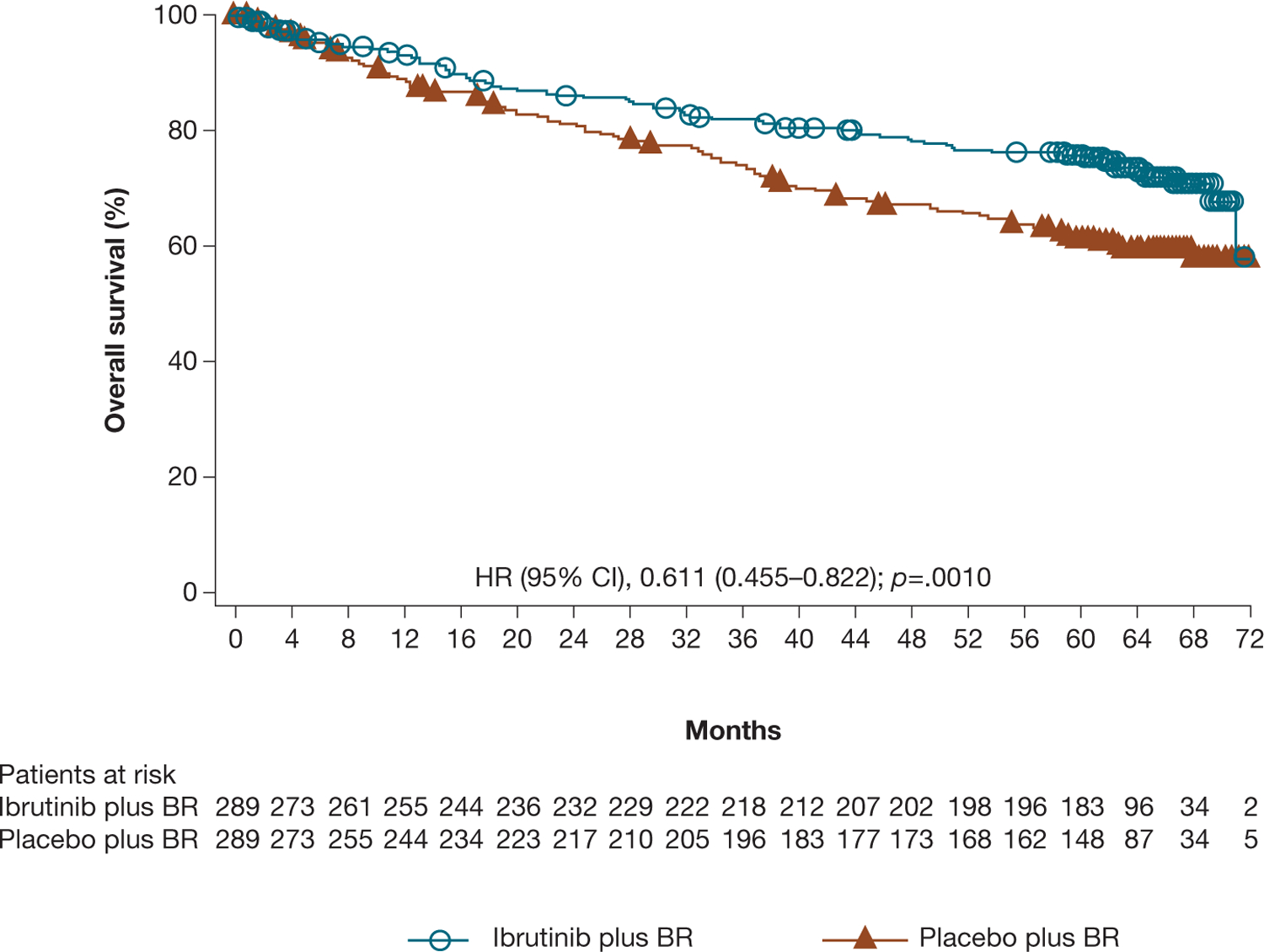
We report final analysis outcomes from the phase 3 HELIOS study (NCT01611090). Patients with relapsed/refractory chronic lymphocytic leukemia/small lymphocytic lymphoma without deletion 17p ( = 578) were randomized 1:1 to 420 mg daily ibrutinib or placebo plus ≤6 cycles of bendamustine plus rituximab (BR), followed by ibrutinib or placebo alone. Median follow-up was 63.7 months. Median investigator-assessed progression-free survival was longer with ibrutinib plus BR (65.1 months) than placebo plus BR (14.3 months; hazard ratio [HR] 0.229 [95% confidence interval (CI) 0.183-0.286]; < .0001). Despite crossover of 63.3% of patients from the placebo plus BR arm to ibrutinib treatment upon disease progression, ibrutinib plus BR versus placebo plus BR demonstrated an overall survival benefit (HR 0.611 [95% CI 0.455-0.822]; = .0010; median not reached in either arm). Long-term follow-up data confirm the survival benefit of ibrutinib plus BR over BR alone. Safety profiles were consistent with those known for ibrutinib and BR.
我们报告了 3 期 HELIOS 研究(NCT01611090)的最终分析结果。无 17p 缺失的复发性/难治性慢性淋巴细胞白血病/小淋巴细胞淋巴瘤患者( = 578)按 1:1 随机分为每日 420mg 伊布替尼或安慰剂加 ≤6 个周期的苯达莫司汀联合利妥昔单抗(BR),随后单独使用伊布替尼或安慰剂。中位随访时间为 63.7 个月。研究者评估的无进展生存期,伊布替尼联合 BR 组(65.1 个月)长于安慰剂联合 BR 组(14.3 个月;危险比 [HR] 0.229 [95%置信区间(CI)0.183-0.286]; < .0001)。尽管有 63.3%的安慰剂联合 BR 组患者在疾病进展后交叉至伊布替尼治疗,但伊布替尼联合 BR 与安慰剂联合 BR 相比显示出总生存获益(HR 0.611 [95%CI 0.455-0.822]; = .0010;两个治疗组的中位无进展生存期均未达到)。长期随访数据证实了伊布替尼联合 BR 比 BR 单药治疗的生存获益。安全性特征与伊布替尼和 BR 已知的安全性特征一致。