Priebe Janosch A, Haas Katharina K, Moreno Sanchez Leida F, Schoefmann Karin, Utpadel-Fischler Daniel A, Stockert Paul, Thoma Reinhard, Schiessl Christine, Kerkemeyer Linda, Amelung Volker, Jedamzik Siegfried, Reichmann Jan, Marschall Ursula, Toelle Thomas R
Center of Interdisciplinary Pain Medicine, Department of Neurology, Klinikum Rechts der Isar, Technical University of Munich, Munich, Germany.
Bayerische TelemedAllianz (BTA), Ingolstadt, Germany.
J Pain Res. 2020 Jul 17;13:1823-1838. doi: 10.2147/JPR.S260761. eCollection 2020.
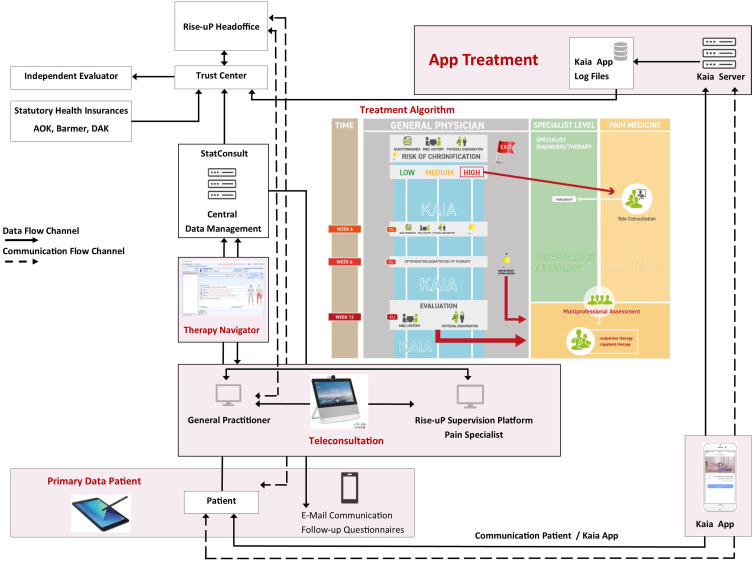
Non-specific low back pain (NLBP) causes an enormous burden to patients and tremendous costs for health care systems worldwide. Frequently, treatments are not oriented to existing guidelines. In the future, digital elements may be promising tools to support guideline-oriented treatment in a broader range of patients. The cluster-randomized controlled "Rise-uP" trial aims to support a General Practitioner (GP)-centered back pain treatment (Registration No: DRKS00015048) and includes the following digital elements: 1) electronic case report form (eCRF), 2) a treatment algorithm for guideline-based clinical decision making of GPs, 3) teleconsultation between GPs and pain specialists for patients at risk for development of chronic back pain, and 4) a multidisciplinary mobile back pain app for all patients (Kaia App).
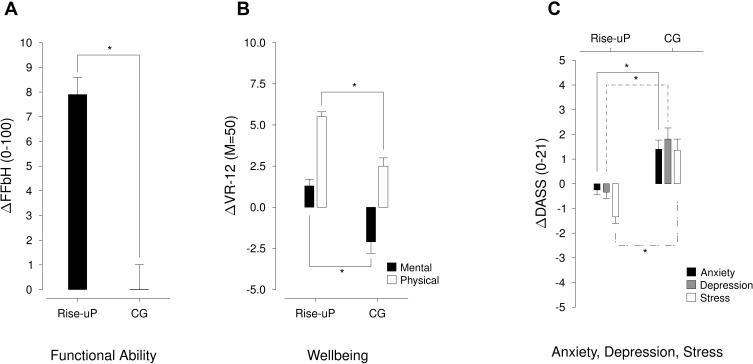
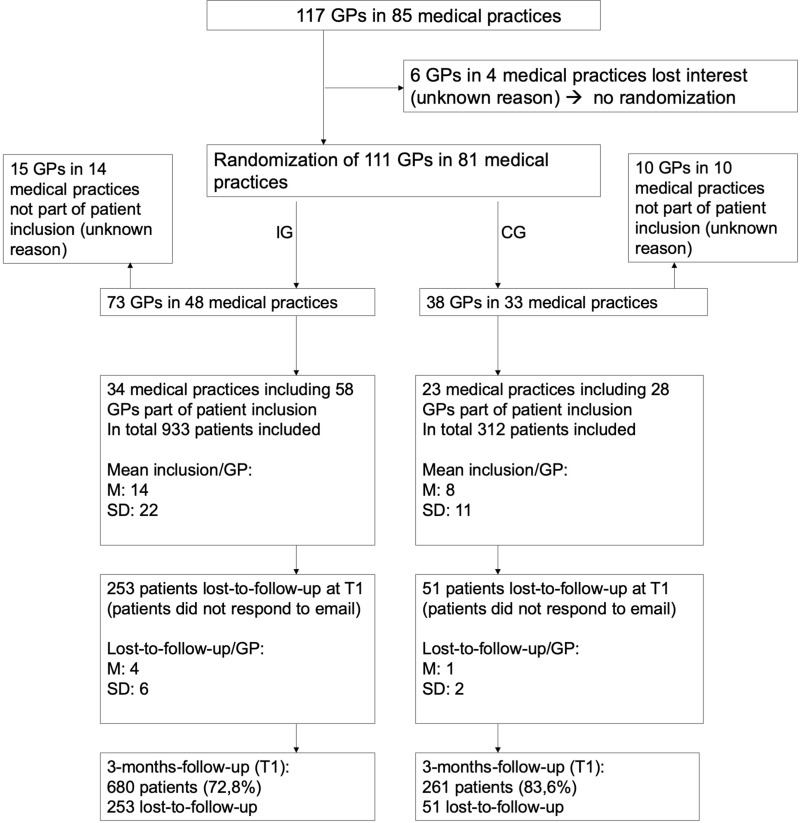
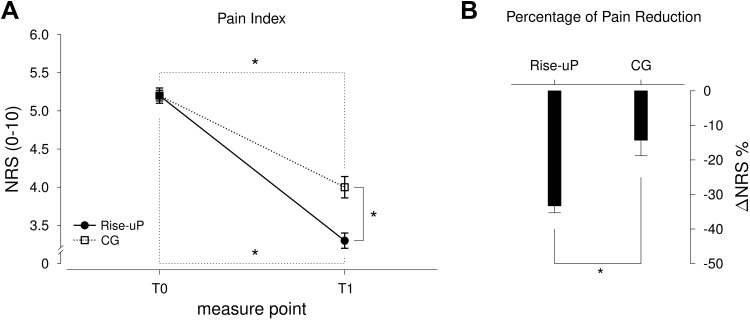
In the Rise-uP trial, 111 GPs throughout Bavaria (southern Germany) were randomized either to the Rise-uP intervention group (IG) or the control group (CG). Rise-uP patients were treated according to the guideline-oriented Rise-uP treatment algorithm. Standard of care was applied to the CG patients with consideration given to the "National guideline for the treatment of non-specific back pain". Pain rating on the numeric rating scale was the primary outcome measure. Psychological measures (anxiety, depression, stress), functional ability, as well as physical and mental wellbeing, served as secondary outcomes. All values were assessed at the beginning of the treatment and at 3-month follow-ups.
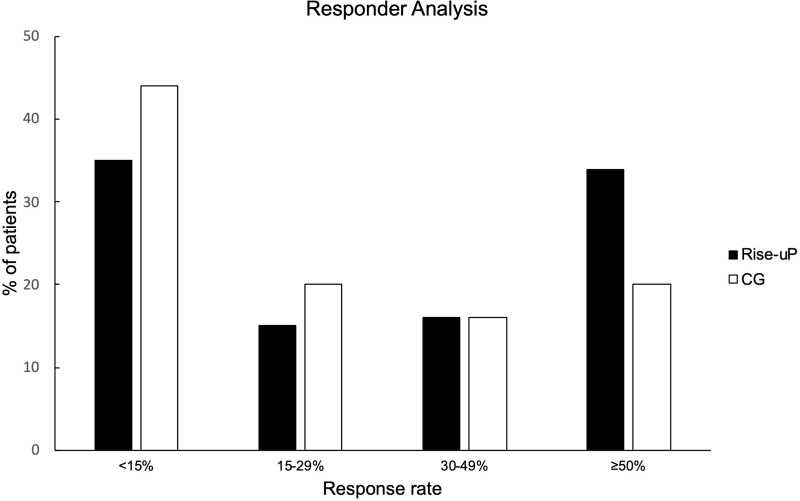
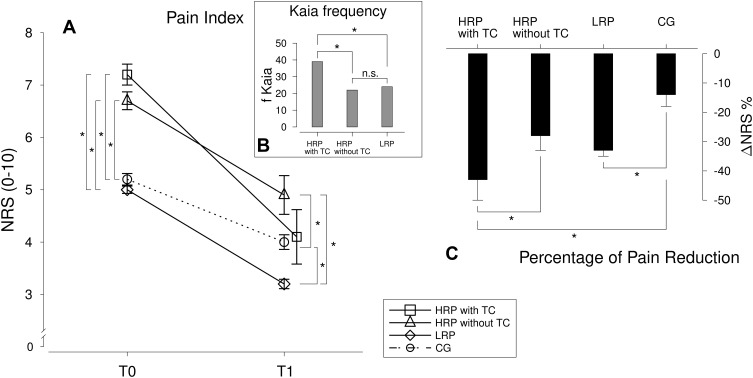
In total, 1245 patients (IG: 933; CG: 312) with NLBP were included in the study. The Rise-uP group showed a significantly stronger pain reduction compared to the control group after 3 months (IG: M=-33.3% vs CG: M=-14.3%). The Rise-uP group was also superior in secondary outcomes. Furthermore, high-risk patients who received a teleconsultation showed a larger decrease in pain intensity (-43.5%) than CG patients (-14.3%). ANCOVA analysis showed that the impact of teleconsultation was mediated by an increased training activity in the Kaia App.
Our results show the superiority of the innovative digital treatment algorithm realized in Rise-uP, even though the CG also received relevant active treatment by their GPs. This provides clear evidence that digital treatment may be a promising tool to improve the quality of treatment of non-specific back pain. In 2021, analyses of routine data from statutory health insurances will enable us to investigate the cost-effectiveness of digital treatment.
非特异性腰痛(NLBP)给患者带来了巨大负担,也给全球医疗保健系统造成了巨大成本。通常,治疗并不遵循现有指南。未来,数字元素可能是支持更广泛患者进行基于指南治疗的有前景的工具。整群随机对照的“Rise-uP”试验旨在支持以全科医生(GP)为中心的腰痛治疗(注册号:DRKS00015048),并包括以下数字元素:1)电子病例报告表(eCRF),2)用于全科医生基于指南的临床决策的治疗算法,3)全科医生与疼痛专家之间针对有慢性背痛发展风险患者的远程会诊,以及4)面向所有患者的多学科移动腰痛应用程序(Kaia应用程序)。
在“Rise-uP”试验中,巴伐利亚州(德国南部)的111名全科医生被随机分为“Rise-uP”干预组(IG)或对照组(CG)。“Rise-uP”患者按照基于指南导向的“Rise-uP”治疗算法进行治疗。对CG组患者采用考虑了“非特异性腰痛治疗国家指南”的标准治疗。数字评分量表上的疼痛评分是主要结局指标。心理测量指标(焦虑、抑郁、压力)、功能能力以及身心健康作为次要结局。所有数值在治疗开始时和3个月随访时进行评估。
该研究共纳入1245例非特异性腰痛患者(IG组:933例;CG组:312例)。3个月后,“Rise-uP”组的疼痛减轻程度明显高于对照组(IG组:M = -33.3%,CG组:M = -14.3%)。“Rise-uP”组在次要结局方面也更具优势。此外,接受远程会诊的高危患者的疼痛强度下降幅度(-43.5%)大于CG组患者(-14.3%)。协方差分析表明,远程会诊的影响是通过增加在Kaia应用程序中的训练活动来介导的。
我们的结果表明,即使CG组患者也从其全科医生那里接受了相关的积极治疗,但“Rise-uP”中实现的创新数字治疗算法仍具有优越性。这提供了明确证据,表明数字治疗可能是提高非特异性腰痛治疗质量的有前景的工具。2021年,对法定医疗保险常规数据的分析将使我们能够研究数字治疗的成本效益。