Kaneko Hiroki, Umakoshi Hironobu, Ishihara Yuki, Nanba Kazutaka, Tsuiki Mika, Kusakabe Toru, Satoh-Asahara Noriko, Yasoda Akihiro, Tagami Tetsuya
Department of Endocrinology and Metabolism, National Hospital Organization Kyoto Medical Center, Kyoto, Japan.
Department of Endocrinology, Metabolism, and Hypertension Research, Clinical Research Institute, National Hospital Organization Kyoto Medical Center, Kyoto, Japan.
J Endocr Soc. 2020 Jul 22;4(9):bvaa100. doi: 10.1210/jendso/bvaa100. eCollection 2020 Sep 1.
Urinary aldosterone levels (Uald) are widely measured in the oral sodium-loading test to confirm primary aldosteronism (PA), but reliable studies on their diagnostic value are limited. This may be due to the difficulty in collecting urine with reliable accuracy, keeping oral sodium intake constant between patients. Therefore, we focused on 24-hour Uald after intravenous saline infusion in a hospitalized setting, which provides a reliable sodium load in consistent amounts.
Comparing plasma aldosterone concentrations (PAC) and Uald after saline infusion in the sitting position, to evaluate the accuracy in determining PA subtypes and the correlation of both measurements.
This was a retrospective cross-sectional study in a single referral center.
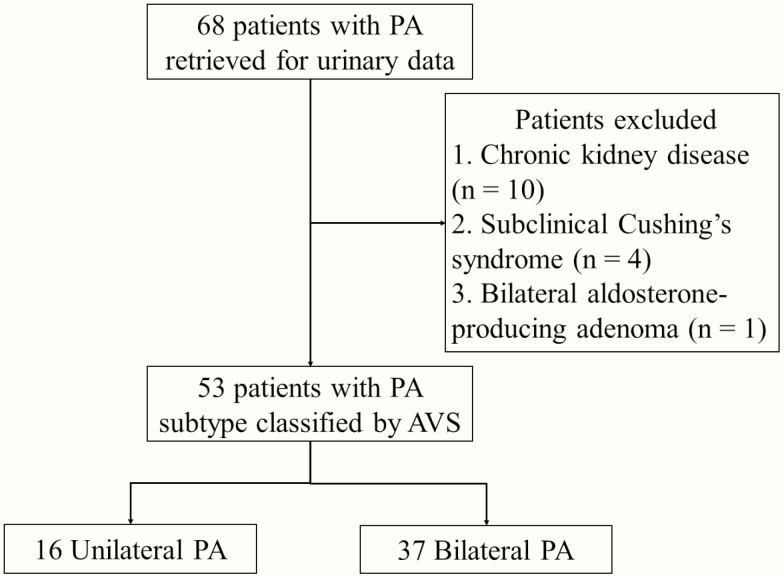
Of 53 patients without renal dysfunction who were diagnosed with PA and underwent adrenal venous sampling, 16 and 37 were diagnosed with unilateral and bilateral PA, respectively.
Uald collected for 24 hours and PAC after saline infusion.
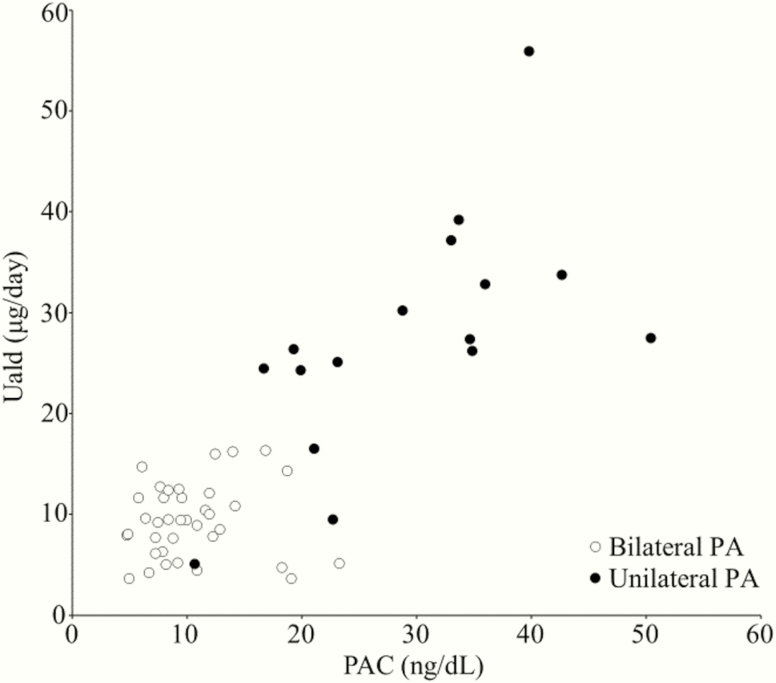
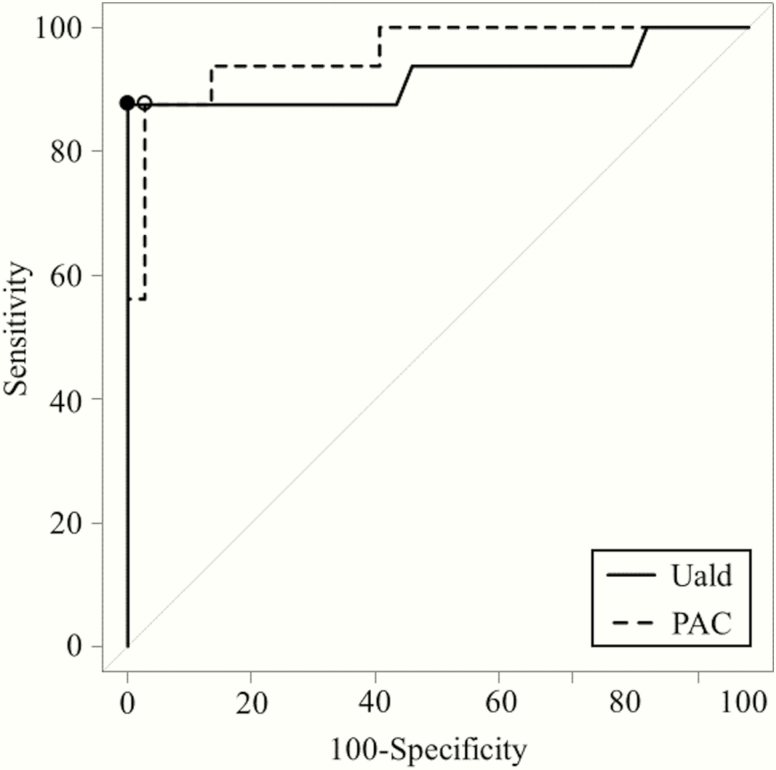
The area under the receiver operating characteristic curve for diagnosing unilateral PA was not significantly different between Uald and PAC after saline infusion (0.921 and 0.958, respectively; = 0.370). The predicted optimal cutoff value of Uald was 16.5 μg/day (sensitivity, 87.5%; specificity, 100%), and that of PAC after saline infusion was 19.3 ng/dL (sensitivity, 87.5%; specificity, 97.3%). In studied patients with PA, Uald was positively correlated with PAC after saline infusion ( = 0.617; < 0.001).
We reassessed Uald in PA patients under sufficient sodium loading and demonstrated the correlation between Uald and PAC after saline infusion.
尿醛固酮水平(Uald)在口服钠负荷试验中被广泛测定以确诊原发性醛固酮增多症(PA),但其诊断价值的可靠研究有限。这可能是由于难以准确可靠地收集尿液,以及患者之间口服钠摄入量难以保持恒定。因此,我们关注住院环境下静脉输注生理盐水后的24小时尿醛固酮水平,其能提供一致量的可靠钠负荷。
比较坐位输注生理盐水后血浆醛固酮浓度(PAC)和尿醛固酮水平,以评估确定PA亚型的准确性以及两种测量方法的相关性。
这是一项在单一转诊中心进行的回顾性横断面研究。
53例无肾功能不全且被诊断为PA并接受肾上腺静脉采血的患者,其中16例和37例分别被诊断为单侧PA和双侧PA。
输注生理盐水后收集的24小时尿醛固酮水平和血浆醛固酮浓度。
输注生理盐水后尿醛固酮水平和血浆醛固酮浓度用于诊断单侧PA的受试者工作特征曲线下面积无显著差异(分别为0.921和0.958;P = 0.370)。尿醛固酮水平的预测最佳截断值为16.5μg/天(敏感性87.5%;特异性100%),输注生理盐水后血浆醛固酮浓度的预测最佳截断值为19.3ng/dL(敏感性87.5%;特异性97.3%)。在研究的PA患者中,尿醛固酮水平与输注生理盐水后的血浆醛固酮浓度呈正相关(r = 0.617;P < 0.001)。
我们在充分钠负荷的PA患者中重新评估了尿醛固酮水平,并证明了输注生理盐水后尿醛固酮水平与血浆醛固酮浓度之间的相关性。