May Alexandra G, Orizondo Ryan A, Frankowski Brian J, Ye Sang-Ho, Kocyildirim Ergin, Wagner William R, D'Cunha Jonathan, Federspiel William J
Department of Chemical and Petroleum Engineering, University of Pittsburgh, Pittsburgh, USA.
McGowan Institute for Regenerative Medicine, University of Pittsburgh, 3025 East Carson Street, Pittsburgh, PA, 15203, USA.
Intensive Care Med Exp. 2020 Aug 17;8(1):45. doi: 10.1186/s40635-020-00329-9.
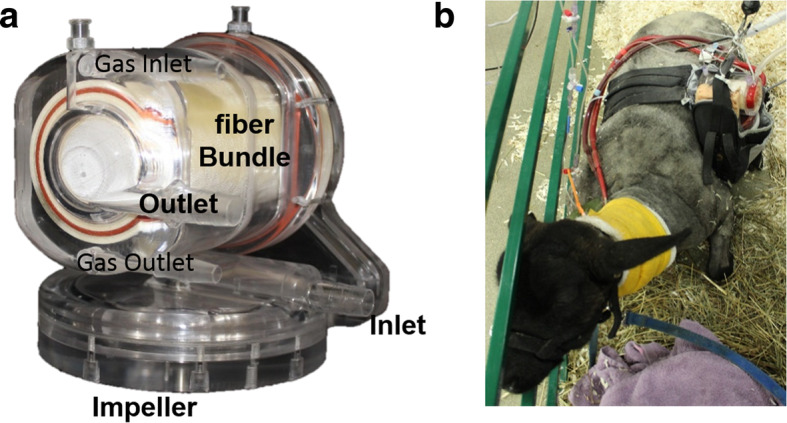
Non-invasive and lung-protective ventilation techniques may improve outcomes for patients with an acute exacerbation of chronic obstructive pulmonary disease or moderate acute respiratory distress syndrome by reducing airway pressures. These less invasive techniques can fail due to hypercapnia and require transitioning patients to invasive mechanical ventilation. Extracorporeal CO removal devices remove CO independent of the lungs thereby controlling the hypercapnia and permitting non-invasive or lung-protective ventilation techniques. We are developing the Modular Extracorporeal Lung Assist System as a platform technology capable of providing three levels of respiratory assist: adult and pediatric full respiratory support and adult low-flow CO removal. The objective of this study was to evaluate the in vivo performance of our device to achieve low-flow CO removal.
The Modular Extracorporeal Lung Assist System was connected to 6 healthy sheep via a 15.5 Fr dual-lumen catheter placed in the external jugular vein. The animals were recovered and tethered within a pen while supported by the device for 7 days. The pump speed was set to achieve a targeted blood flow of 500 mL/min. The extracorporeal CO removal rate was measured daily at a sweep gas independent regime. Hematological parameters were measured pre-operatively and regularly throughout the study. Histopathological samples of the end organs were taken at the end of each study.
All animals survived the surgery and generally tolerated the device well. One animal required early termination due to a pulmonary embolism. Intra-device thrombus formation occurred in a single animal due to improper anticoagulation. The average CO removal rate (normalized to an inlet pCO of 45 mmHg) was 75.6 ± 4.7 mL/min and did not significantly change over the course of the study (p > 0.05). No signs of consistent hemolysis or end organ damage were observed.
These in vivo results indicate positive performance of the Modular Extracorporeal Lung Assist System as a low-flow CO removal device.
无创和肺保护性通气技术可通过降低气道压力改善慢性阻塞性肺疾病急性加重或中度急性呼吸窘迫综合征患者的预后。这些侵入性较小的技术可能因高碳酸血症而失败,需要将患者转为有创机械通气。体外二氧化碳清除装置可独立于肺清除二氧化碳,从而控制高碳酸血症,并允许采用无创或肺保护性通气技术。我们正在开发模块化体外肺辅助系统作为一种平台技术,能够提供三级呼吸支持:成人和儿童的全呼吸支持以及成人低流量二氧化碳清除。本研究的目的是评估我们的设备在实现低流量二氧化碳清除方面的体内性能。
通过置于颈外静脉的15.5 Fr双腔导管将模块化体外肺辅助系统连接到6只健康绵羊。动物恢复后,在围栏内用该设备支撑7天。将泵速设置为达到500 mL/min的目标血流。在独立于吹扫气体的状态下每日测量体外二氧化碳清除率。术前及研究期间定期测量血液学参数。在每项研究结束时采集终末器官的组织病理学样本。
所有动物均在手术后存活,且对该设备总体耐受性良好。1只动物因肺栓塞需要提前终止实验。1只动物因抗凝不当在设备内形成血栓。平均二氧化碳清除率(归一化为入口pCO为45 mmHg)为75.6±4.7 mL/min,在研究过程中无显著变化(p>0.05)。未观察到持续溶血或终末器官损伤的迹象。
这些体内结果表明模块化体外肺辅助系统作为低流量二氧化碳清除设备具有良好性能。