Emory Clinical Cardiovascular Research Institute, Division of Cardiology, Department of Medicine, Emory University School of Medicine, Atlanta, GA (A.M., L.S.S.).
Division of Cardiology, Department of Internal Medicine (A.P., A.K., P.H.J.), University of Texas Southwestern Medical Center, Dallas.
Circ Cardiovasc Imaging. 2020 Aug;13(8):e010153. doi: 10.1161/CIRCIMAGING.119.010153. Epub 2020 Aug 18.
Coronary artery calcium (CAC) predicts atherosclerotic cardiovascular disease (ASCVD) events, inclusive of coronary heart disease (CHD) and stroke, and is a decision-making aid for primary prevention. The predictive value of CAC categories for CHD and stroke separately and across sex and race groups of an asymptomatic population is unclear.
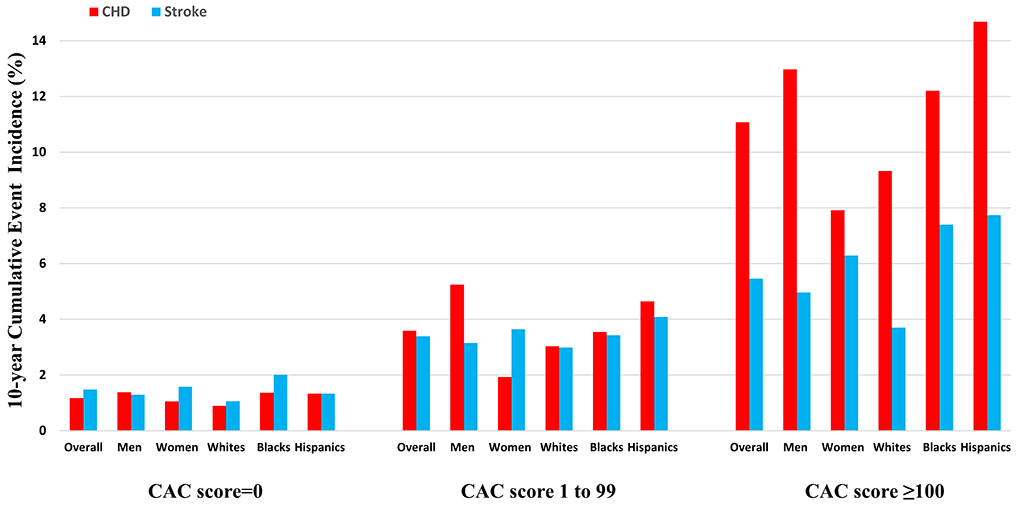
White, Black, and Hispanic participants of MESA (Multi-Ethnic Study of Atherosclerosis) and DHS (Dallas Heart Study) underwent CAC measurement at enrollment and were followed for incident ASCVD events. Ten-year CHD-to-stroke incidence ratios across CAC score categories 0, 1 to 99, and ≥100 were assessed. Associations of CAC with incident CHD and stroke events were evaluated using multivariable-adjusted Cox models and multiplicative interactions of CAC with sex/race were tested.
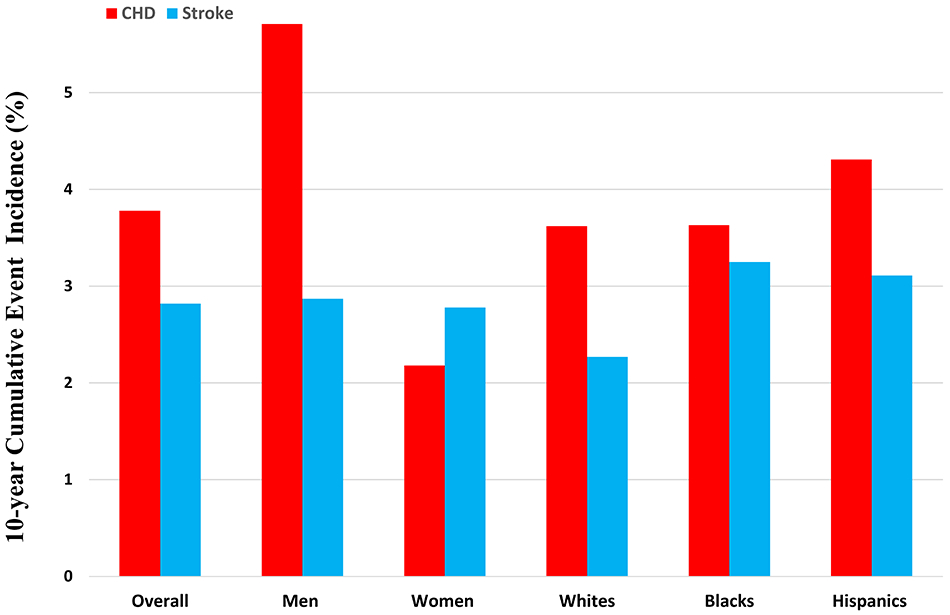
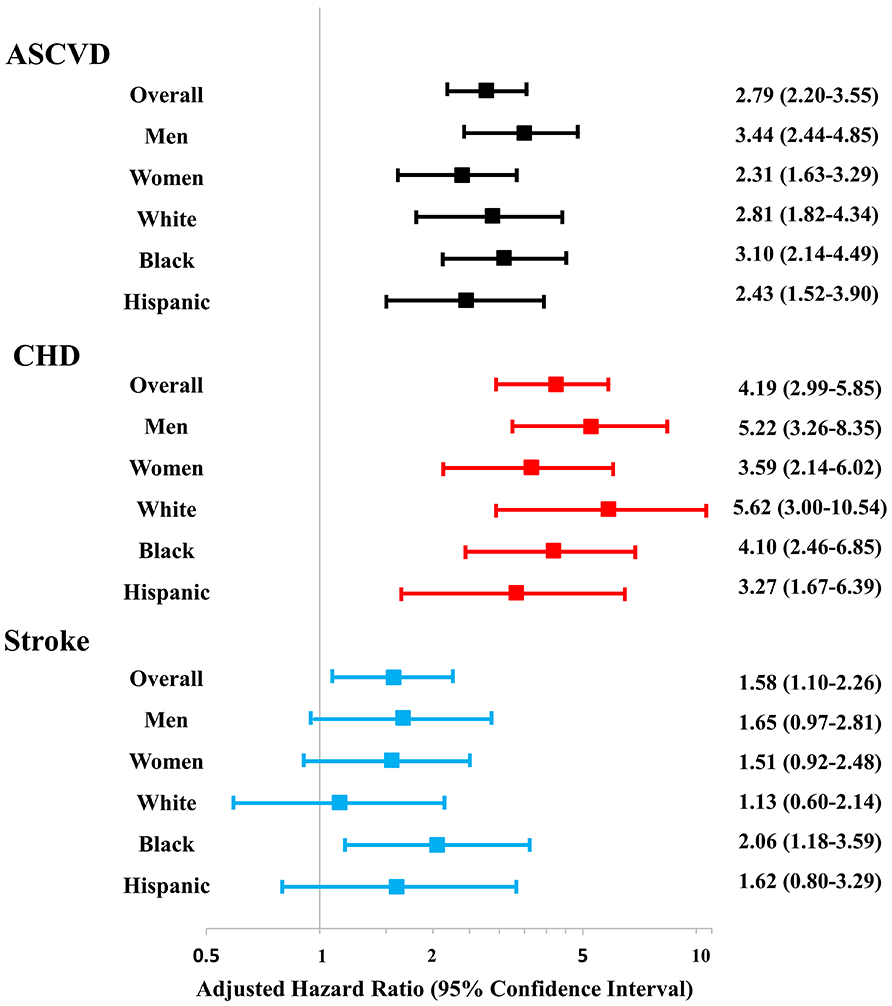
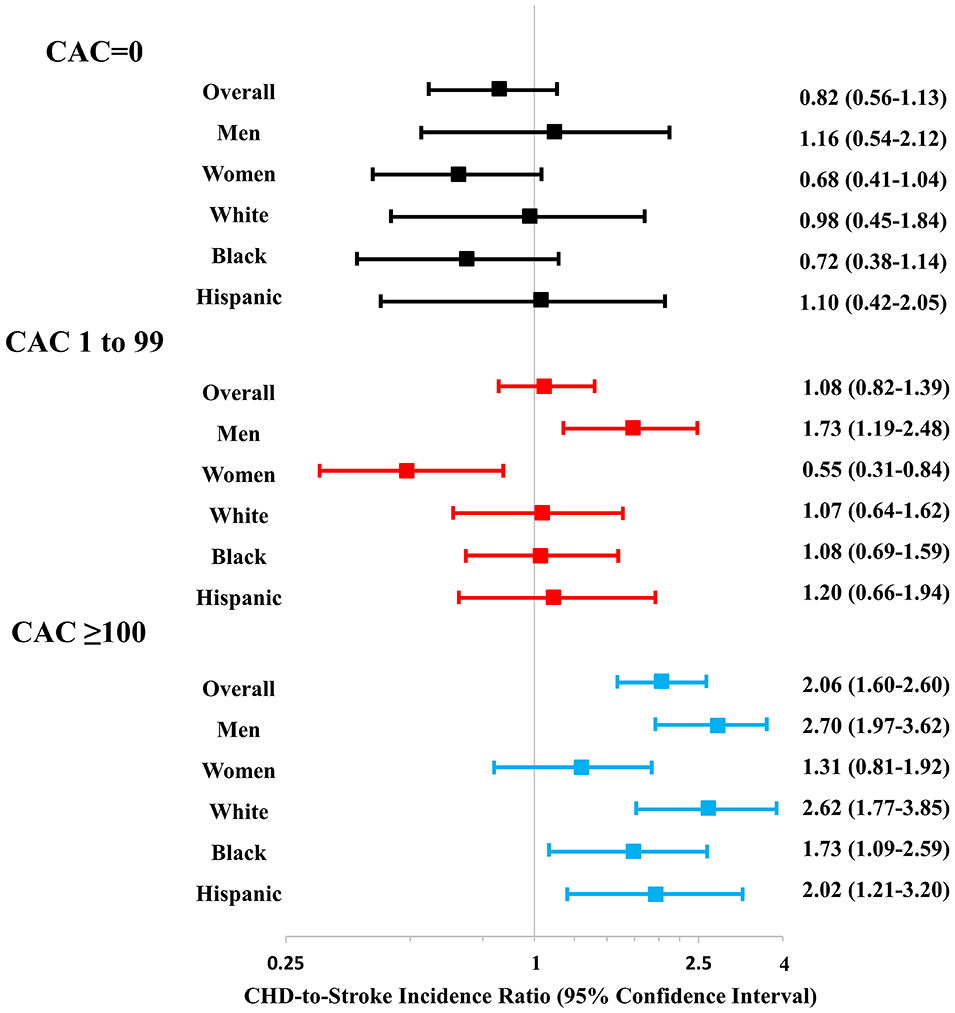
Among 7042 participants (mean age, 57 years, 54% women, 36% Black, 23% Hispanic, 49% CAC=0, 19% CAC ≥100), 574 incident ASCVD events (333 CHD and 241 stroke) were observed over 12.3-year follow-up. Ten-year CHD-to-stroke incidence ratio increased significantly across CAC categories in men, women, Whites, Blacks, and Hispanics (all <0.001). High CAC burden (score ≥100) was independently associated with ASCVD and CHD risk in all groups and with stroke risk in the overall cohort and Blacks. No sex- or race-based CAC interactions for ASCVD, CHD, and stroke events were observed. Adding CAC to a traditional risk factor model improved risk discrimination and reclassification for CHD but not for stroke events.
In 2 population-based cohorts of asymptomatic individuals, 10-year CHD-to-stroke incidence ratio was higher with increasing CAC score categories across sex and race groups, and CAC was consistently a better predictor of CHD than stroke. High CAC burden comparably associated with ASCVD risk across sex and race groups.
冠状动脉钙(CAC)可预测动脉粥样硬化性心血管疾病(ASCVD)事件,包括冠心病(CHD)和中风,是一级预防的决策辅助工具。无症状人群中 CAC 类别对 CHD 和中风的预测价值,以及在不同性别和种族群体中的预测价值尚不清楚。
MESA(多民族动脉粥样硬化研究)和 DHS(达拉斯心脏研究)的白种人、黑人和西班牙裔参与者在入组时进行 CAC 测量,并随访 ASCVD 事件的发生情况。评估 CAC 评分 0、1 至 99 和≥100 分的 10 年 CHD 至中风发生率比。使用多变量调整 Cox 模型评估 CAC 与 CHD 和中风事件的相关性,并测试 CAC 与性别/种族的相乘交互作用。
在 7042 名参与者(平均年龄 57 岁,54%为女性,36%为黑人,23%为西班牙裔,49%的 CAC=0,19%的 CAC≥100)中,在 12.3 年的随访期间观察到 574 例 ASCVD 事件(333 例 CHD 和 241 例中风)。在男性、女性、白种人、黑人和西班牙裔中,CAC 类别显著增加,10 年 CHD 至中风的发生率比值也随之显著增加(均<0.001)。高 CAC 负担(评分≥100)与所有组的 ASCVD 和 CHD 风险以及整个队列和黑人的中风风险独立相关。未观察到 ASCVD、CHD 和中风事件的基于性别或种族的 CAC 相互作用。将 CAC 添加到传统风险因素模型中可改善 CHD 的风险区分和再分类,但不能改善中风事件的风险区分和再分类。
在 2 个基于人群的无症状个体队列中,随着 CAC 评分类别的增加,男女和种族群体的 10 年 CHD 至中风发生率比值更高,而 CAC 始终是 CHD 的更好预测因子,而不是中风。高 CAC 负担与男女和种族群体的 ASCVD 风险相当相关。