Nephrology, Dialysis and Transplantation Unit, Careggi University Hospital, Florence, Italy.
Department of Medicine and Surgery, University of Parma, Parma, Italy; Geriatric-Rehabilitation Department, Parma University Hospital, Parma, Italy.
Ultrasound Med Biol. 2020 Nov;46(11):2908-2917. doi: 10.1016/j.ultrasmedbio.2020.07.018. Epub 2020 Jul 20.
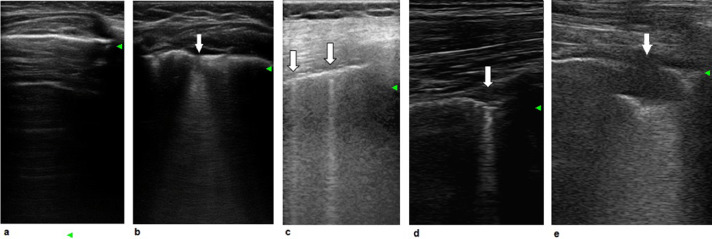
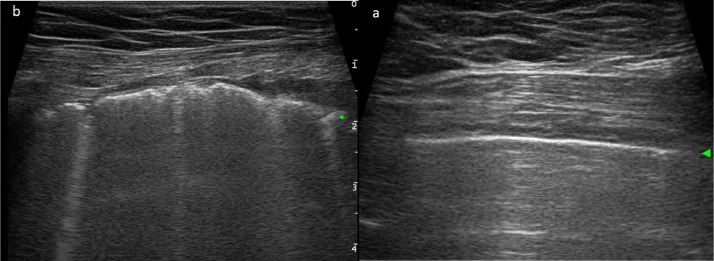
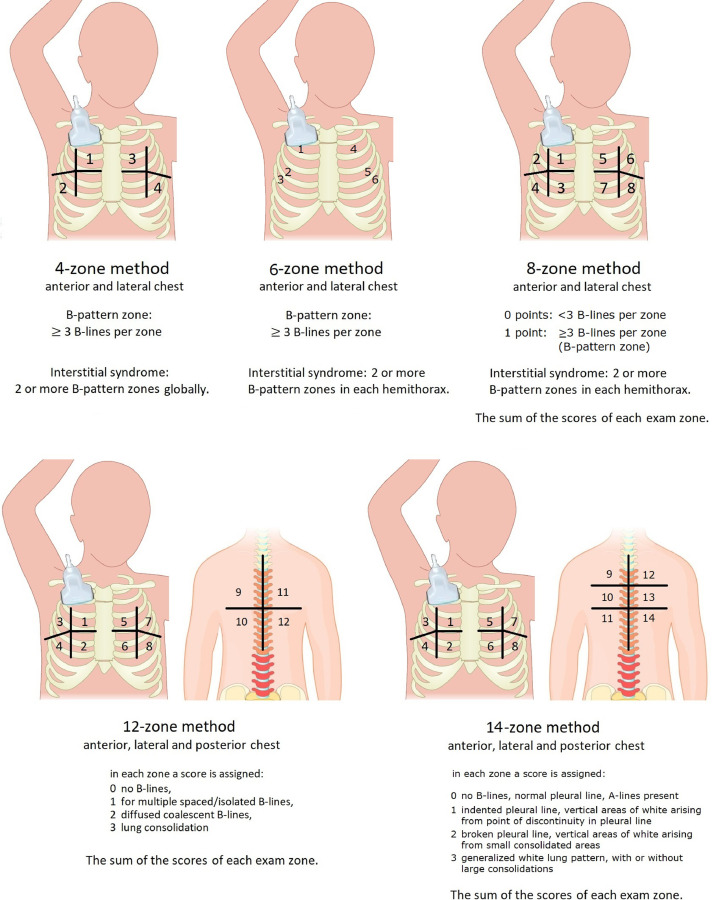
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) disease (COVID-19) is characterized by severe pneumonia and/or acute respiratory distress syndrome in about 20% of infected patients. Computed tomography (CT) is the routine imaging technique for diagnosis and monitoring of COVID-19 pneumonia. Chest CT has high sensitivity for diagnosis of COVID-19, but is not universally available, requires an infected or unstable patient to be moved to the radiology unit with potential exposure of several people, necessitates proper sanification of the CT room after use and is underutilized in children and pregnant women because of concerns over radiation exposure. The increasing frequency of confirmed COVID-19 cases is striking, and new sensitive diagnostic tools are needed to guide clinical practice. Lung ultrasound (LUS) is an emerging non-invasive bedside technique that is used to diagnose interstitial lung syndrome through evaluation and quantitation of the number of B-lines, pleural irregularities and nodules or consolidations. In patients with COVID-19 pneumonia, LUS reveals a typical pattern of diffuse interstitial lung syndrome, characterized by multiple or confluent bilateral B-lines with spared areas, thickening of the pleural line with pleural line irregularity and peripheral consolidations. LUS has been found to be a promising tool for the diagnosis of COVID-19 pneumonia, and LUS findings correlate fairly with those of chest CT scan. Compared with CT, LUS has several other advantages, such as lack of exposure to radiation, bedside repeatability during follow-up, low cost and easier application in low-resource settings. Consequently, LUS may decrease utilization of conventional diagnostic imaging resources (CT scan and chest X-ray). LUS may help in early diagnosis, therapeutic decisions and follow-up monitoring of COVID-19 pneumonia, particularly in the critical care setting and in pregnant women, children and patients in areas with high rates of community transmission.
严重急性呼吸综合征冠状病毒 2(SARS-CoV-2)疾病(COVID-19)的特征是约 20%的感染患者患有严重肺炎和/或急性呼吸窘迫综合征。计算机断层扫描(CT)是 COVID-19 肺炎诊断和监测的常规成像技术。胸部 CT 对 COVID-19 的诊断具有很高的敏感性,但并非普遍可用,需要将感染或不稳定的患者转移到放射科单位,可能会使多人暴露,需要在使用后对 CT 室进行适当的消毒,并且由于对辐射暴露的担忧,在儿童和孕妇中未得到充分利用。确诊 COVID-19 病例的频率不断增加,需要新的敏感诊断工具来指导临床实践。肺部超声(LUS)是一种新兴的非侵入性床边技术,用于通过评估和量化 B 线数量、胸膜不规则和结节或实变来诊断间质性肺综合征。在 COVID-19 肺炎患者中,LUS 显示出弥漫性间质性肺综合征的典型模式,其特征是双侧多个或融合的 B 线,伴有未受累区域,胸膜线增厚伴胸膜不规则和外周实变。已经发现 LUS 是 COVID-19 肺炎诊断的一种很有前途的工具,并且 LUS 发现与胸部 CT 扫描相当。与 CT 相比,LUS 具有其他几个优点,例如无辐射暴露、在随访期间可床边重复、成本低且易于在资源有限的环境中应用。因此,LUS 可能会减少对常规诊断成像资源(CT 扫描和胸部 X 射线)的利用。LUS 可能有助于 COVID-19 肺炎的早期诊断、治疗决策和随访监测,特别是在重症监护环境中和孕妇、儿童和社区传播率高的地区的患者中。