Amgen (Europe) GmbH, Global Health Economics, Suurstoffi 22, 6343, Rotkreuz, Switzerland.
Amgen Inc, Global Health Economics, Thousand Oaks, CA, USA.
Pharmacoeconomics. 2020 Nov;38(11):1219-1236. doi: 10.1007/s40273-020-00952-0.
Heart failure presents a growing clinical and economic burden in the USA. Robust cost data on the burden of illness are critical to inform economic evaluations of new therapeutic interventions.
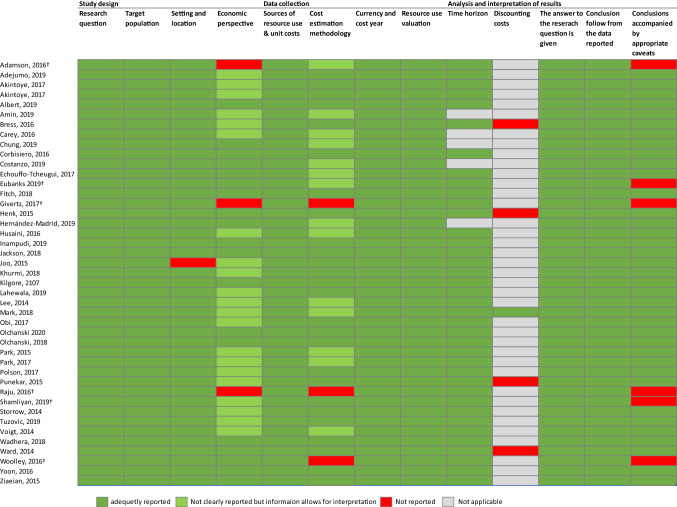
This systematic literature review of heart failure-related costs in the USA aimed to assess the quality of the published evidence and provide a narrative synthesis of current data.
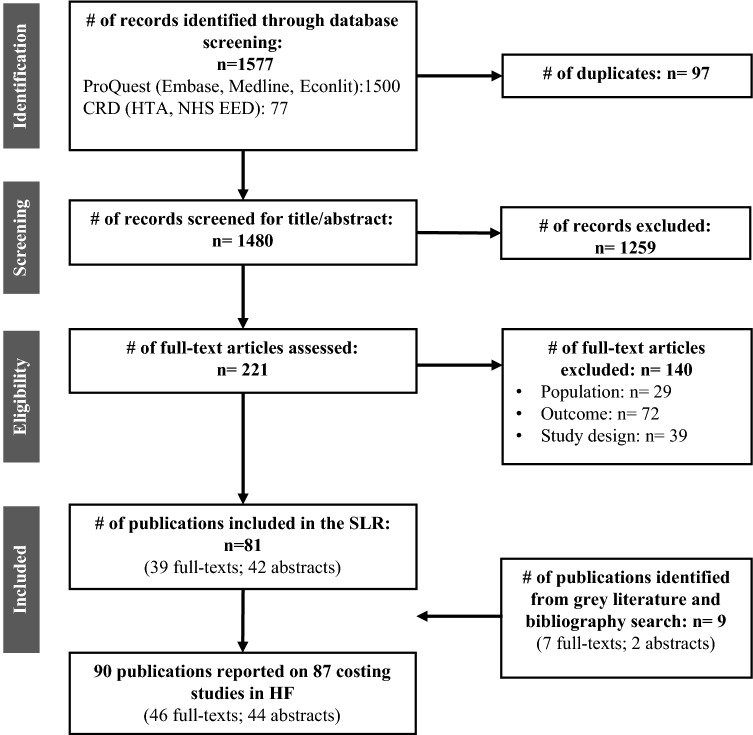
Four electronic databases (MEDLINE, EMBASE, EconLit, and the Centre for Reviews and Dissemination York Database, including the NHS Economic Evaluation Database and Health Technology Assessment Database) were searched for journal articles published between January 2014 and March 2020. The review, registered with PROSPERO (CRD42019134201), was restricted to cost-of-illness studies in adults with heart failure events in the USA.
Eighty-seven studies were included, 41 of which allowed a comparison of cost estimates across studies. The annual median total medical costs for heart failure care were estimated at $24,383 per patient, with heart failure-specific hospitalizations driving costs (median $15,879 per patient). Analyses of subgroups revealed that heart failure-related costs are highly sensitive to individual patient characteristics (such as the presence of comorbidities and age) with large variations even within a subgroup. Additionally, differences in study design and a lack of standardized reporting limited the ability to compare cost estimates. The finding that costs are higher for patients with heart failure with reduced ejection fraction compared with patients with preserved ejection fraction highlights the need for differentiating among different heart failure types.
The review underpins the conclusion drawn in earlier reviews, namely that hospitalization costs are the key driver of heart failure-related costs. Analyses of subgroups provide a clearer understanding of sources of heterogeneity in cost data. While current cost estimates provide useful indications of economic burden, understanding the nuances of the data is critical to support its application.
心力衰竭在美国带来了日益增长的临床和经济负担。有关疾病负担的可靠成本数据对于新治疗干预措施的经济评估至关重要。
本系统评价旨在评估美国心力衰竭相关成本的文献质量,并对现有数据进行叙述性综合分析。
检索了四个电子数据库(MEDLINE、EMBASE、EconLit 和约克大学评论与传播中心数据库,包括英国国家卫生与保健优化研究所经济评价数据库和卫生技术评估数据库),以获取 2014 年 1 月至 2020 年 3 月期间发表的与心力衰竭相关的美国成人成本的期刊文章。本综述(在 PROSPERO 注册,CRD42019134201)仅限于美国心力衰竭事件的成本效益研究。
共纳入 87 项研究,其中 41 项研究允许对研究间的成本估算进行比较。心力衰竭患者的年平均医疗总成本估计为每位患者 24383 美元,心力衰竭特定住院治疗导致的费用(每位患者 15879 美元)最高。亚组分析表明,心力衰竭相关成本对个体患者特征(如合并症和年龄)高度敏感,即使在亚组内也存在较大差异。此外,研究设计的差异以及缺乏标准化报告限制了对成本估算的比较。与射血分数保留的心力衰竭患者相比,射血分数降低的心力衰竭患者的心力衰竭相关成本更高,这突出表明需要区分不同类型的心力衰竭。
本综述支持早期综述得出的结论,即住院费用是心力衰竭相关费用的主要驱动因素。亚组分析提供了对成本数据异质性来源的更清晰理解。尽管目前的成本估算提供了对经济负担的有用指示,但理解数据的细微差别对于支持其应用至关重要。