DSI-NRF Centre of Excellence in Epidemiological Modelling and Analysis (SACEMA), Stellenbosch University, Stellenbosch, South Africa; Desmond Tutu TB Centre, Department of Paediatrics and Child Health, Faculty of Medicine and Health Sciences, Stellenbosch University, Cape Town, South Africa.
Department of Epidemiology of Microbial Diseases, Yale School of Public Health, New Haven, CT, USA.
Lancet Glob Health. 2020 Sep;8(9):e1223-e1233. doi: 10.1016/S2214-109X(20)30227-8.
In settings of high tuberculosis incidence, previously treated individuals remain at high risk of recurrent tuberculosis and contribute substantially to overall disease burden. Whether tuberculosis case finding and preventive interventions among previously treated people are cost-effective has not been established. We aimed to estimate costs and health benefits of annual post-treatment follow-up examinations and secondary preventive therapy for tuberculosis in a tuberculosis-endemic setting.
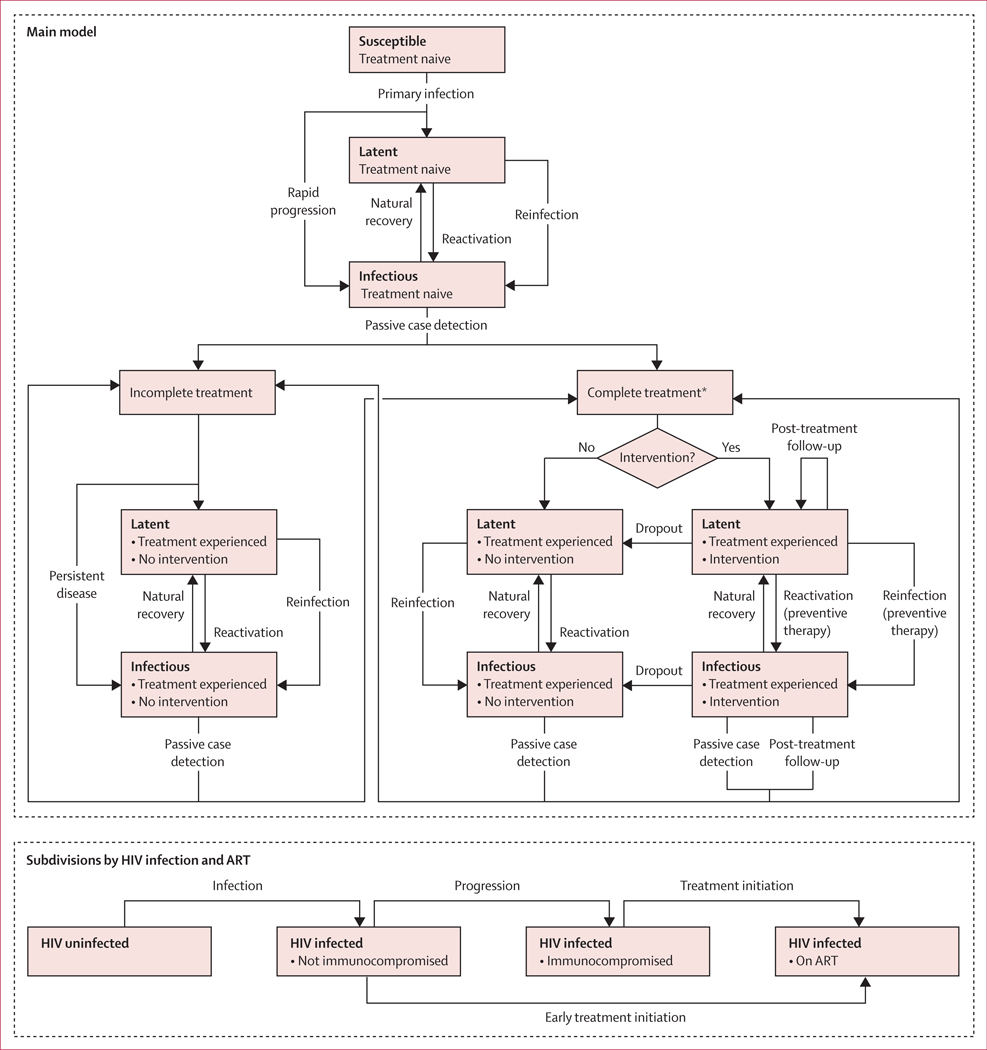
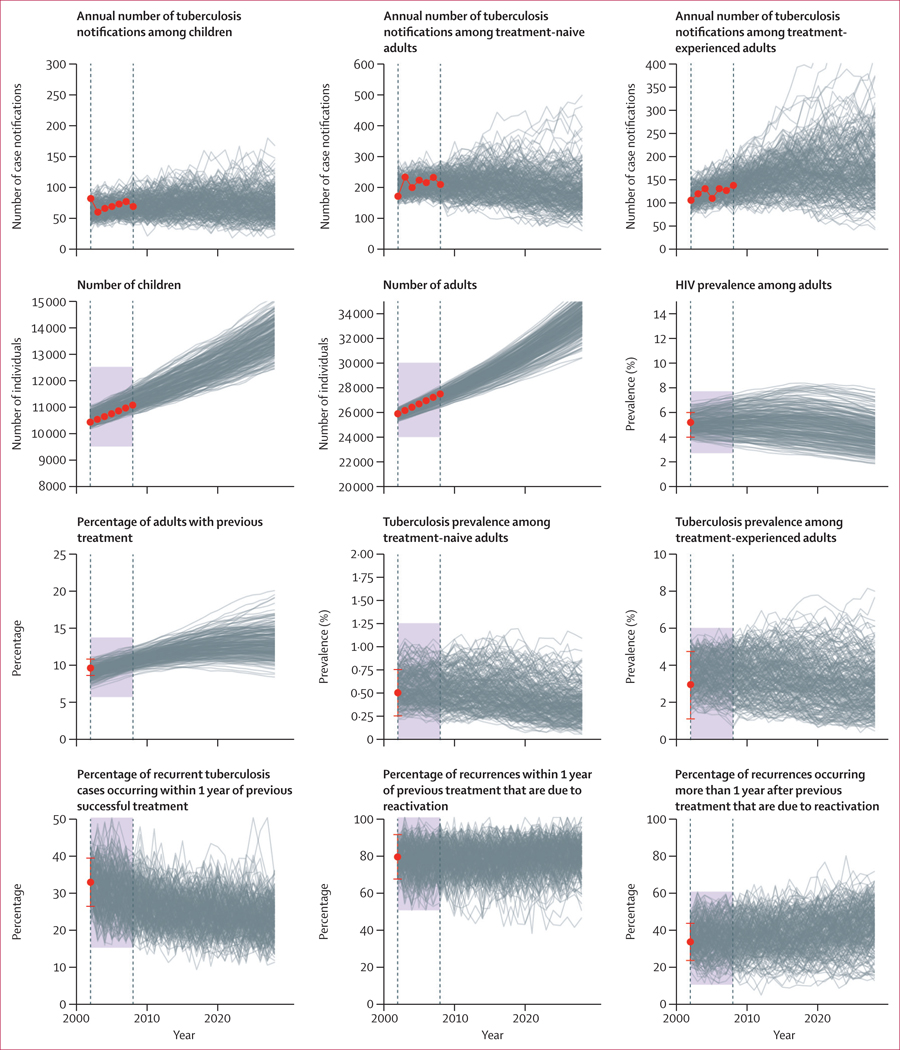
We developed a transmission-dynamic mathematical model and calibrated it to data from two high-incidence communities of approximately 40 000 people in suburban Cape Town, South Africa. We used the model to estimate overall cost and disability-adjusted life-years (DALYs) associated with annual follow-up examinations and secondary isoniazid preventive therapy (IPT), alone and in combination, among individuals completing tuberculosis treatment. We investigated scenarios under which these interventions were restricted to the first year after treatment completion, or extended indefinitely. For each intervention scenario, we projected health system costs and DALYs averted with respect to the current status quo of tuberculosis control. All estimates represent mean values derived from 1000 epidemic trajectories simulated over a 10-year period (2019-28), with 95% uncertainty intervals (UIs) calculated as the 2·5th and 97·5th percentile values.
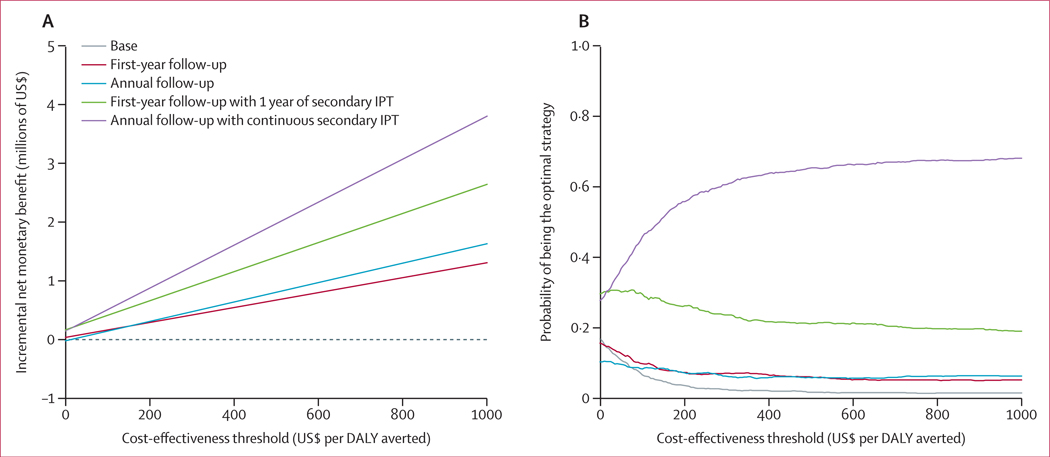
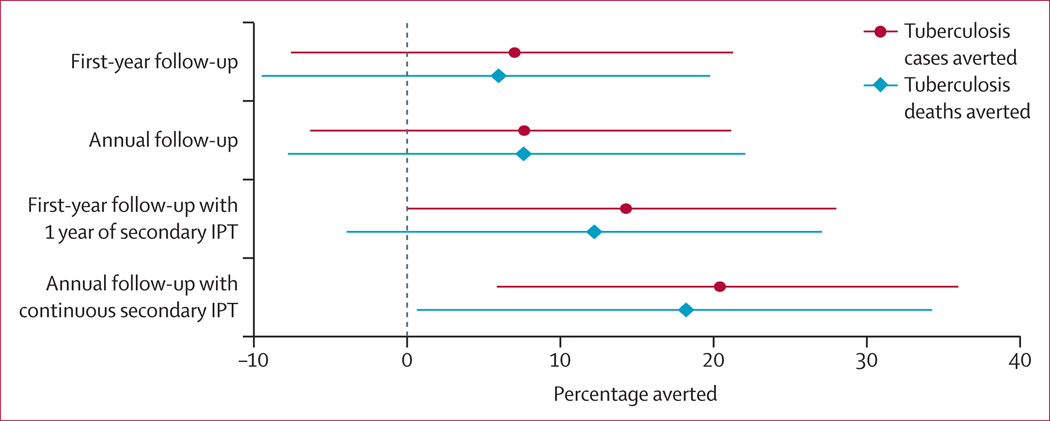
We estimated that a single follow-up examination at the end of the first year after treatment completion combined with 12 months of secondary IPT would avert 2472 DALYs (95% UI -888 to 7801) over a 10-year period and is expected to be cost-saving compared with current control efforts. Sustained annual follow-up and continuous secondary IPT beyond the first year after treatment would avert an additional 1179 DALYs (-1769 to 4377) over 10 years at an expected additional cost of US$18·2 per DALY averted. Strategies of follow-up without secondary IPT were dominated (ie, expected to result in lower health impact at higher costs) by strategies that included secondary IPT.
In this high-incidence setting, post-treatment follow-up and secondary preventive therapy can accelerate declines in tuberculosis incidence and potentially save resources for tuberculosis control. Empirical trials to assess the feasibility of these interventions in settings most severely affected by tuberculosis are needed.
National Institutes of Health, Günther Labes Foundation, Oskar Helene Heim Foundation.
在结核病高发地区,既往治疗过的个体仍面临较高的复发性结核病风险,并对整体疾病负担做出了重大贡献。既往治疗人群中发现结核病病例和实施预防性干预措施是否具有成本效益尚不清楚。本研究旨在估算在结核病流行地区,对既往治疗人群进行年度治疗后随访检查和二线异烟肼预防性治疗的成本和健康获益。
我们构建了一个基于传播动力学的数学模型,并使用来自南非开普敦郊区两个约 4 万人的高发病率社区的数据进行了校准。我们利用该模型估算了单独开展以及联合开展年度随访检查和二线异烟肼预防性治疗(IPT)在完成结核病治疗的个体中,与年度随访检查和二线 IPT 相关的总体成本和伤残调整生命年(DALYs)。我们研究了这些干预措施仅在治疗完成后的第一年实施或无限期延长的情景。对于每种干预方案,我们都根据目前的结核病控制现状,预测了卫生系统成本和避免的 DALYs。所有估计值均为通过在 10 年内(2019-2028 年)模拟 1000 条流行轨迹得到的平均值,95%置信区间(UI)为第 2.5 百分位数和第 97.5 百分位数的范围。
我们估计,在治疗完成后第一年的年末进行一次随访检查,并联合开展 12 个月的二线 IPT,可在 10 年内避免 2472 个 DALYs(95%UI -888 至 7801),与目前的控制努力相比预计具有成本效益。在治疗完成后的第一年之后持续进行年度随访和连续二线 IPT,在 10 年内可额外避免 1179 个 DALYs(-1769 至 4377),预计每避免一个 DALY 需额外花费 18.2 美元。没有二线 IPT 的随访策略(即预计会以更高的成本产生更低的健康影响),被包含二线 IPT 的策略所主导。
在这个高发病率地区,治疗后随访和二级预防治疗可以加速结核病发病率的下降,并可能为结核病控制节省资源。需要开展评估这些干预措施在受结核病影响最严重地区的可行性的实证性试验。
美国国立卫生研究院、Günther 实验室基金会、Oskar Helene Heim 基金会。