Department of Anesthesia and Critical Care, Hospital of the University of Pennsylvania, University of Pennsylvania, Philadelphia, PA.
Division of Cardiovascular Surgery, Department of Surgery, Hospital of the University of Pennsylvania, University of Pennsylvania, Philadelphia, PA.
J Cardiothorac Vasc Anesth. 2020 Nov;34(11):3006-3012. doi: 10.1053/j.jvca.2020.07.063. Epub 2020 Jul 28.
Anticoagulation may be a challenge in coronavirus disease 2019 (COVID-19) extracorporeal membrane oxygenation due to endothelial injury and dysregulation of coagulation, which may increase the risk of thrombotic and bleeding complications. This report was created to describe the authors' single institutional experience, with emphasis on the high rate of intracranial hemorrhage for the first 10 patients with COVID-19 placed on venovenous extracorporeal membrane oxygenation (VV ECMO).
Case series, retrospective analysis.
Single institution.
Ten patients.
None.
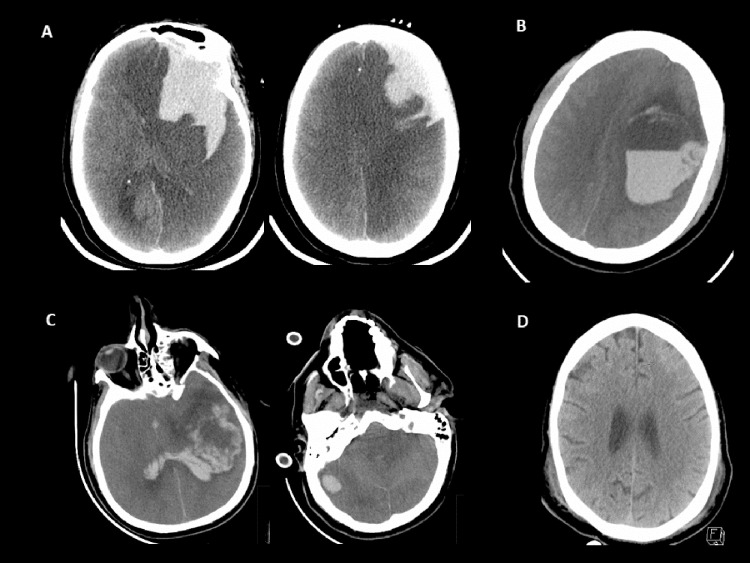
Patient characteristics, mortality, stroke rate, and length of stay data were collected in all patients. In addition, laboratory values of D-dimer and C-reactive protein and standard measurements of prothrombin and activated partial thromboplastin time were collected on all patients. Ten patients, each confirmed with COVID-19 via reverse transcription-polymerase chain reaction, were supported on VV ECMO for acute respiratory distress syndrome (ARDS) for a mean duration of 9.4 ± 7 days. Four of 10 patients had hemorrhagic strokes, 3 of which resulted in death. At 30 days after initiation of VV ECMO, a total of 7 survivors included 6 patients discharged from the hospital and 1 patient who remained in the intensive care unit.
In this small study of 10 patients, intracranial hemorrhage was a common complication, resulting in a high rate of death. The authors urge caution in the anticoagulation management of VV ECMO for patients with severe ARDS and COVID-19 patients. Close monitoring of all hematologic parameters is recommended during ECMO support while awaiting larger, multicenter studies to examine the best practice.
由于内皮损伤和凝血失调,COVID-19 体外膜肺氧合(ECMO)可能会给抗凝带来挑战,这可能会增加血栓形成和出血并发症的风险。本报告旨在描述作者所在机构的单中心经验,重点是前 10 名 COVID-19 患者接受静脉-静脉 ECMO(VV ECMO)治疗的颅内出血发生率较高。
病例系列,回顾性分析。
单机构。
10 名患者。
无。
收集了所有患者的患者特征、死亡率、卒中发生率和住院时间数据。此外,还收集了所有患者的 D-二聚体和 C 反应蛋白的实验室值以及凝血酶原和活化部分凝血活酶时间的标准测量值。10 名患者均通过逆转录-聚合酶链反应(RT-PCR)确诊为 COVID-19,接受 VV ECMO 治疗急性呼吸窘迫综合征(ARDS),平均持续时间为 9.4 ± 7 天。10 名患者中有 4 名发生了出血性卒中,其中 3 例死亡。在开始 VV ECMO 治疗后 30 天,7 名幸存者中共有 6 名患者出院,1 名患者仍在重症监护病房。
在这项对 10 名患者的小型研究中,颅内出血是一种常见的并发症,导致死亡率较高。作者敦促在严重 ARDS 和 COVID-19 患者中对 VV ECMO 的抗凝管理保持谨慎。在 ECMO 支持期间,建议密切监测所有血液学参数,同时等待更大规模的多中心研究来检查最佳实践。