Oliveros Henry, Buitrago Giancarlo
Department of Clinical Epidemiology and Biostatistics, Pontificia Universidad Javeriana, Bogotá, Colombia.
School of Medicine, Universidad de la Sabana, Autonorte de Bogota Km 7, La Caro, Chía, Colombia.
J Intensive Care. 2020 Aug 18;8:63. doi: 10.1186/s40560-020-00481-0. eCollection 2020.
Between 30 and 70% of patients admitted to the intensive care unit (ICU) have acute kidney injury (AKI), and 10% of these patients will require renal replacement therapy (RRT). A significant number of studies have compared the mortality of patients who require RRT versus those who do not require it, finding an increase in mortality rates in the short and medium term; however, few studies have evaluated the long-term survival in a mixture of patients admitted to the ICU.
To evaluate the impact of RRT on 5-year survival in patients with AKI admitted to the ICU.
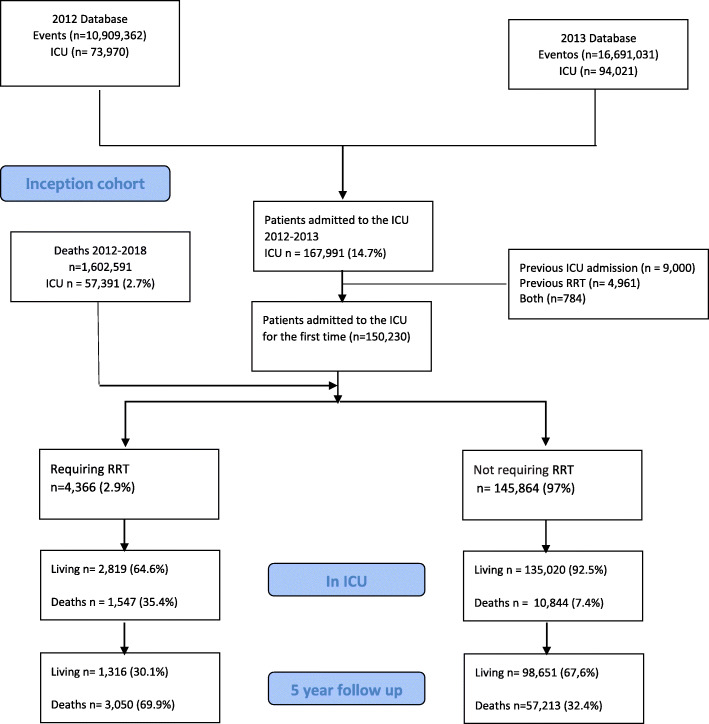
Using administrative databases of insurers of the Colombian health system, a cohort of patients admitted to the ICU between 1 January 2012 and 31 December 2013 was followed until 31 December 2018. ICD-10 diagnoses, procedure codes, and prescribed medications were used to establish the frequencies of the comorbidities included in the Charlson index. Patients were followed for at least 5 years to evaluate survival and establish the adjusted risks by propensity score matching.
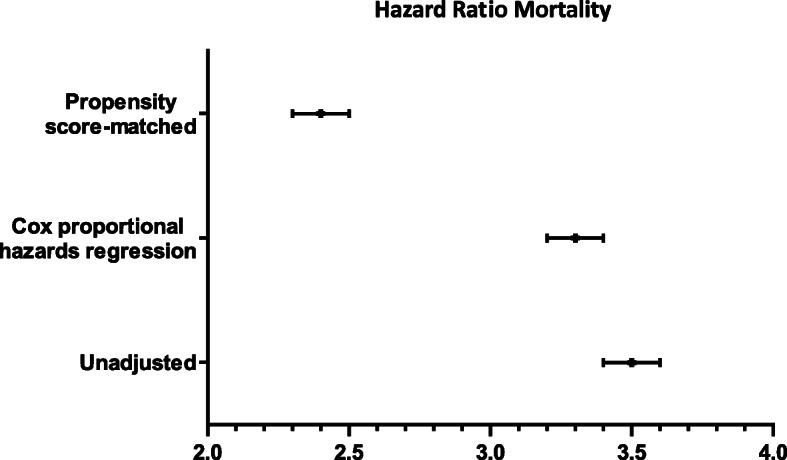
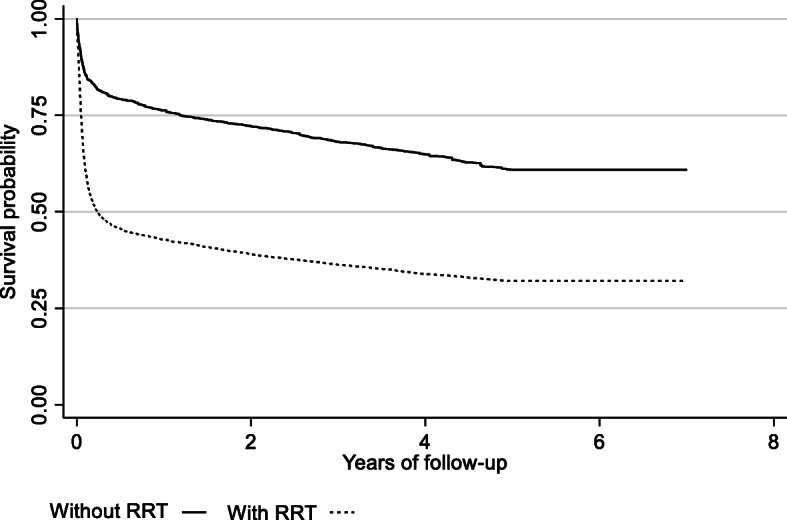
Of the 150,230 patients admitted to the ICU, 4366 (2.9%) required RRT in the ICU. Mortality rates for patients with RRT vs no RRT evaluated at ICU discharge, 1 year, and 5 years were 35%, 57.4%, and 67.9% vs 7.4%, 17.6%, and 30.1%, respectively. After propensity score matching, the hazard ratio was calculated for patients who received RRT and those who did not (HR, 2.46; 95% CI 2.37 to 2.56; < 0.001), with a lower difference in years of survival for patients with RRT (mean effect in the treated) of - 1.86 (95% CI - 2.01 to to1.65; < 0.001).
The impact of acute renal failure with the consequent need for RRT in patients admitted to the ICU is reflected in a decrease of approximately one quarter in 5-year survival, regardless of the different comorbidities.
入住重症监护病房(ICU)的患者中,30%至70%患有急性肾损伤(AKI),其中10%的患者需要肾脏替代治疗(RRT)。大量研究比较了需要RRT的患者与不需要RRT的患者的死亡率,发现短期和中期死亡率有所增加;然而,很少有研究评估入住ICU的混合患者的长期生存率。
评估RRT对入住ICU的AKI患者5年生存率的影响。
利用哥伦比亚卫生系统保险公司的行政数据库,对2012年1月1日至2013年12月31日期间入住ICU的一组患者进行随访,直至2018年12月31日。使用国际疾病分类第十版(ICD - 10)诊断、手术编码和处方药物来确定Charlson指数中合并症的发生率。对患者进行至少5年的随访,以评估生存率,并通过倾向评分匹配确定调整后的风险。
在150230例入住ICU的患者中,4366例(2.9%)在ICU需要RRT。在ICU出院时、1年和5年时评估,需要RRT的患者与不需要RRT的患者的死亡率分别为35%、57.4%和67.9%,而后者分别为7.4%、17.6%和30.1%。经过倾向评分匹配后,计算接受RRT的患者与未接受RRT的患者的风险比(HR,2.46;95%可信区间2.37至2.56;P < 0.001),接受RRT的患者生存年数差异较小(治疗组的平均效应)为 - 1.86(95%可信区间 - 2.01至 - 1.65;P < 0.001)。
入住ICU的患者因急性肾衰竭而需要RRT,这对5年生存率的影响是使其降低约四分之一,无论合并症情况如何。