Üstünyurt Emin
University of Health Sciences Turkey, Bursa Yüksek İhtisas Training and Research Hospital, Clinic of Gynecology, Bursa, Turkey.
Turk J Obstet Gynecol. 2020 Jun;17(2):108-114. doi: 10.4274/tjod.galenos.2020.82652. Epub 2020 Jul 29.
Placenta accreta spectrum (PAS) is a potentially life-threatening condition characterized by the abnormal adherence of the placenta to the implantation site. We sought to evaluate the efficacy, surgical feasibility, risks, and advantages of local uterine resection in cases complicated with PAS.
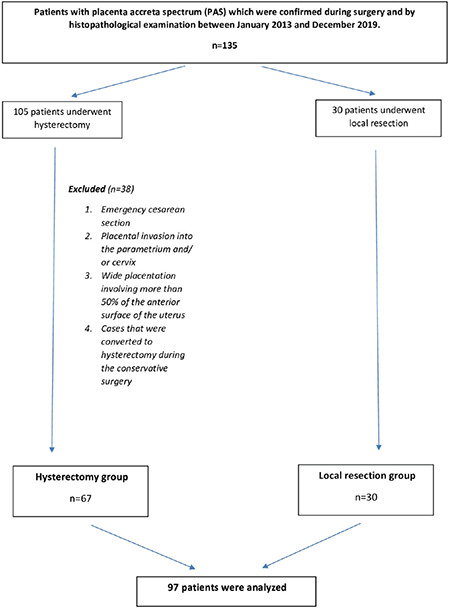
This study included 97 patients with PAS, which was confirmed during surgery and by histopathological examination between January 2013 and December 2019. The patients were divided into two groups based on operative approach. The study population (local resection group) consisted of 30 cases in whom total resection of adherent placenta and myometrium was performed, whereas the control group (hysterectomy group) of 67 cesarean hysterectomy cases.
Patients who underwent hysterectomy had significantly more bleeding than the local resection group (1180±160 mL vs 877±484 mL; p=0.002). The mean number of transfused packed red blood cells (pRBCs) was greater in the hysterectomy group (4.5±2.3) than in the local resection group (2.6±3.1; p=0.001). Transfusion rate of four and/or more pRBCs was 67.2% in the hysterectomy group and 33.3% in the local resection group, which indicated a statistically significant difference (p=0.002). Of patients, 29.6% required intensive care unit in the hysterectomy group and 6.7% in the local resection group (p=0.023).
Local resection can be performed safely in selected PAS cases. In these cases, using a standardized protocol in terms of patient selection and surgical procedure will reduce morbidity and mortality.
胎盘植入谱系疾病(PAS)是一种潜在的危及生命的疾病,其特征是胎盘异常附着于着床部位。我们旨在评估局部子宫切除术在合并PAS病例中的疗效、手术可行性、风险及优势。
本研究纳入了97例PAS患者,这些患者在2013年1月至2019年12月期间经手术及组织病理学检查确诊。根据手术方式将患者分为两组。研究组(局部切除术组)包括30例患者,对其进行了附着胎盘及子宫肌层的全切除,而对照组(子宫切除术组)为67例行剖宫产子宫切除术的病例。
接受子宫切除术的患者出血量明显多于局部切除术组(1180±160 mL对877±484 mL;p = 0.002)。子宫切除术组输注浓缩红细胞(pRBC)的平均数量(4.5±2.3)多于局部切除术组(2.6±3.1;p = 0.001)。子宫切除术组输注4个及以上pRBC的输血率为67.2%,局部切除术组为33.3%,差异有统计学意义(p = 0.002)。子宫切除术组29.6%的患者需要入住重症监护病房,局部切除术组为6.7%(p = 0.023)。
在选定的PAS病例中可安全地进行局部切除术。在这些病例中,在患者选择和手术操作方面采用标准化方案将降低发病率和死亡率。