Koster Andreas, Nazy Ishac, Birschmann Ingvild E, Smith James W, Sheppard Jo-Ann I, Warkentin Theodore E
Institute of Anesthesiology and Pain Therapy, Heart and Diabetes Center NRW Ruhr-University Bochum Bad Oeynhausen Germany.
Department of Medicine Michael G. DeGroote School of Medicine McMaster University Hamilton ON Canada.
Res Pract Thromb Haemost. 2020 Jul 23;4(6):1060-1064. doi: 10.1002/rth2.12348. eCollection 2020 Aug.
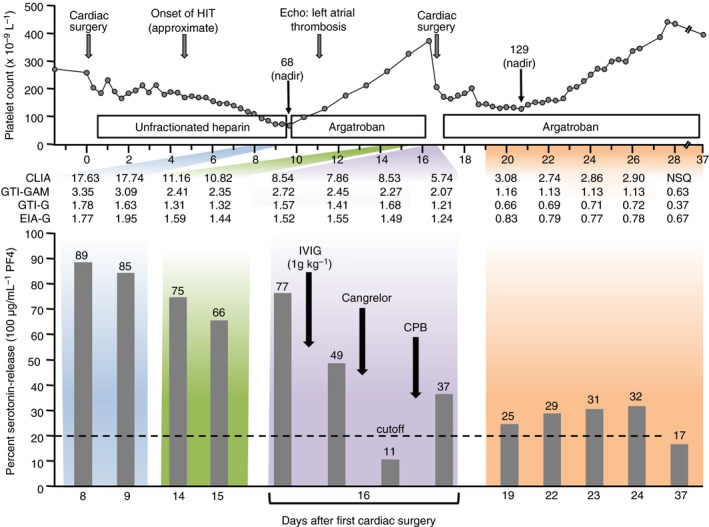
In a high-risk patient with subacute heparin-induced thrombocytopenia (HIT) type A (platelet count recovery following acute HIT but with persisting platelet-activating antibodies), in whom urgent cardiac surgery was required, a key clinical question arose: could intraoperative heparin be given safely with "platelet anesthesia" provided with high-dose intravenous immunoglobulin (IVIG) plus cangrelor (ultra-short-acting antiplatelet agent)? This approach proved successful, without unexpected postoperative thrombocytopenia or thromboembolism. In vitro studies confirmed that both IVIG and cangrelor contributed to perioperative inhibition of HIT antibody-induced platelet activation. Interestingly, despite the patient testing strongly positive in 4 HIT immunoassays (latex immunoturbidimetric assay and 3 enzyme-immunoassays), the serotonin-release assay (SRA) was consistently negative. Nevertheless, platelet-activating HIT antibodies were detectable using modified (platelet factor 4-enhanced) SRA. Our protocol of heparin rechallenge following IVIG/cangrelor provides both intraoperative and early postoperative inhibition of HIT antibody-induced platelet activation and is applicable to patients with circulating functional HIT antibodies requiring urgent heart surgery, including those with "SRA-negative HIT."
在一名患有A型亚急性肝素诱导的血小板减少症(HIT)的高风险患者中(急性HIT后血小板计数恢复,但血小板激活抗体持续存在),该患者需要紧急心脏手术,由此产生了一个关键的临床问题:在给予高剂量静脉注射免疫球蛋白(IVIG)加坎格雷洛(超短效抗血小板药物)进行“血小板麻醉”的情况下,术中能否安全给予肝素?这种方法被证明是成功的,术后没有出现意外的血小板减少或血栓栓塞。体外研究证实,IVIG和坎格雷洛都有助于围手术期抑制HIT抗体诱导的血小板激活。有趣的是,尽管该患者在4种HIT免疫测定(乳胶免疫比浊法和3种酶免疫测定)中检测结果均为强阳性,但血清素释放试验(SRA)始终为阴性。然而,使用改良的(血小板因子4增强的)SRA可检测到血小板激活的HIT抗体。我们在IVIG/坎格雷洛之后重新使用肝素的方案可在术中和术后早期抑制HIT抗体诱导的血小板激活,适用于需要紧急心脏手术的循环功能性HIT抗体患者,包括那些“血清素释放试验阴性的HIT”患者。