Department of Radiation Oncology (Maastro), GROW School for Oncology, Maastricht University Medical Centre+, Maastricht, The Netherlands.
Department of Medical Oncology, GROW School for Oncology, Maastricht University Medical Centre+, Maastricht, The Netherlands.
Autophagy. 2021 Sep;17(9):2604-2612. doi: 10.1080/15548627.2020.1816343. Epub 2020 Sep 20.
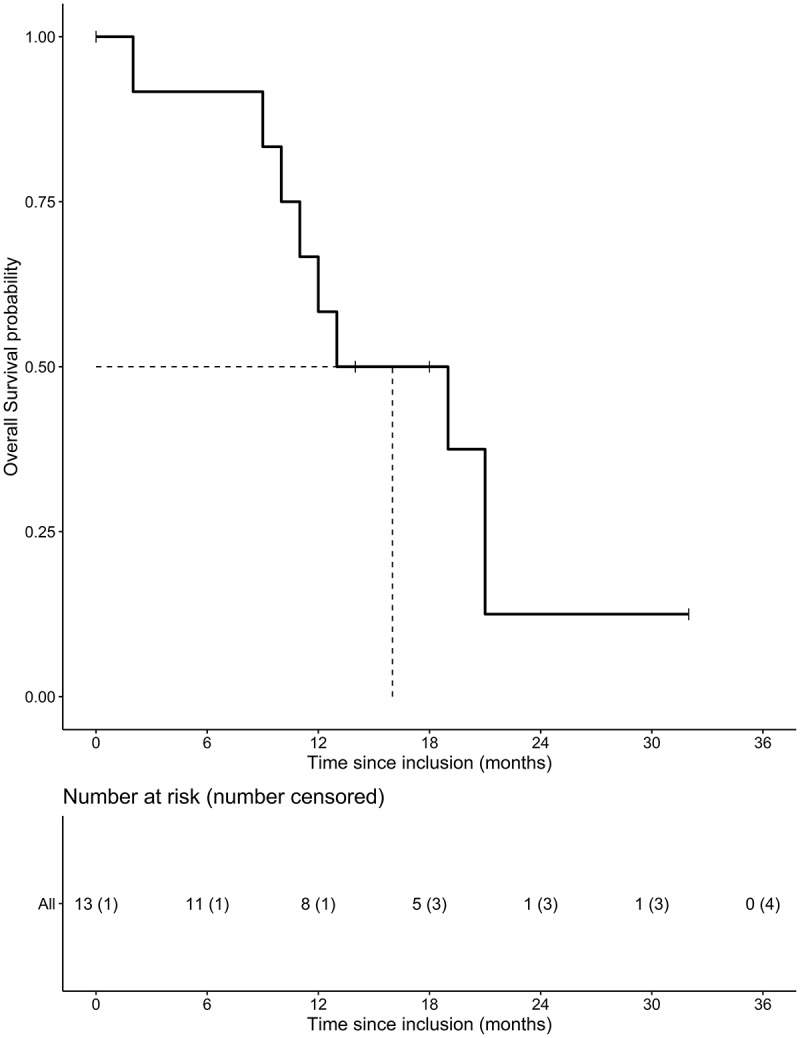
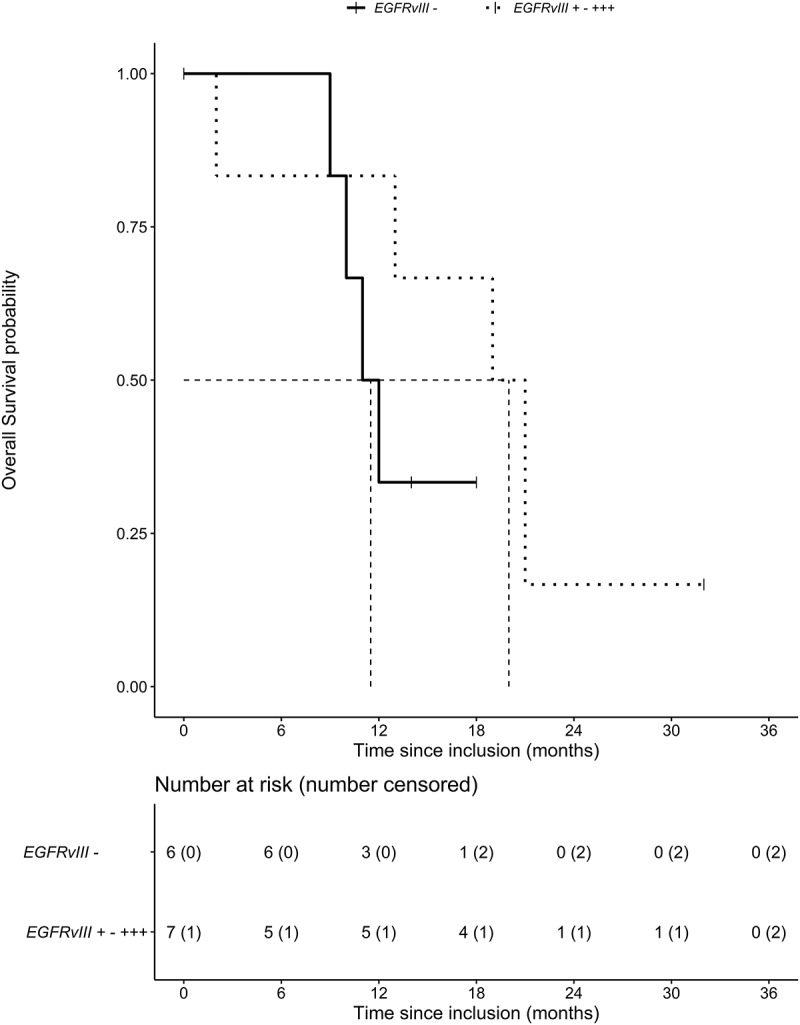
Treatment of glioblastoma xenografts with chloroquine results in macroautophagy/autophagy inhibition, resulting in a reduction of tumor hypoxia and sensitization to radiation. Preclinical data show that -expressing glioblastoma may benefit most from chloroquine because of autophagy dependency. This study is the first to explore the safety, pharmacokinetics and maximum tolerated dose of chloroquine in combination with radiotherapy and concurrent daily temozolomide in patients with a newly diagnosed glioblastoma. This study is a single-center, open-label, dose-finding phase I trial. Patients received oral chloroquine daily starting one week before the course of chemoradiation (temozolomide 75 mg/m/d) until the end of radiotherapy (59.4 Gy/33 fractions). Thirteen patients were included in the study (n = 6: 200 mg, n = 3: 300 mg, n = 4: 400 mg chloroquine). A total of 44 adverse events, possibly related to chloroquine, were registered including electrocardiogram QTc prolongation, irreversible blurred vision and nausea/vomiting resulting in cessation of temozolomide or delay of adjuvant cycles. The maximum tolerated dose was 200 mg chloroquine. Median overall survival was 16 months (range 2-32). Median survival was 11.5 months for - patients and 20 months for + patients. A daily dose of 200 mg chloroquine was determined to be the maximum tolerated dose when combined with radiotherapy and concurrent temozolomide for newly diagnosed glioblastoma. Favorable toxicity and promising overall survival support further clinical studies. AE: adverse events; CQ: chloroquine; DLT: dose-limiting toxicities; EGFR: epidermal growth factor receptor; GBM: glioblastoma; HCQ: hydroxychloroquine; : isocitrate dehydrogenase (NADP(+)) 1/2; MTD: maximum tolerated dose; CTC: National Cancer Institute Common Toxicity Criteria; : O-6-methylguanine-DNA methyltransferase; OS: overall survival; po qd: per os quaque die; SAE: serious adverse events; TMZ: temozolomide; WHO: World Health Organization.
氯喹治疗神经胶质瘤异种移植物导致巨自噬/自噬抑制,从而减少肿瘤缺氧并增加对放射治疗的敏感性。临床前数据表明,表达的神经胶质瘤可能从氯喹中获益最大,因为它依赖于自噬。本研究首次探索了氯喹联合放疗和同期每日替莫唑胺治疗新诊断的胶质母细胞瘤患者的安全性、药代动力学和最大耐受剂量。这是一项单中心、开放性、剂量递增的 I 期临床试验。患者在放化疗(替莫唑胺 75mg/m/d)疗程前一周开始每天口服氯喹,直至放疗结束(59.4Gy/33 次)。本研究共纳入 13 例患者(n=6:200mg,n=3:300mg,n=4:400mg 氯喹)。共登记了 44 例可能与氯喹相关的不良事件,包括心电图 QTc 延长、不可逆的视力模糊和恶心/呕吐,导致替莫唑胺停药或辅助周期延迟。最大耐受剂量为 200mg 氯喹。中位总生存期为 16 个月(范围 2-32)。-患者的中位生存期为 11.5 个月,+患者的中位生存期为 20 个月。当与放疗和同期替莫唑胺联合用于新诊断的胶质母细胞瘤时,确定 200mg 氯喹为最大耐受剂量。良好的毒性和有希望的总生存期支持进一步的临床研究。AE:不良事件;CQ:氯喹;DLT:剂量限制毒性;EGFR:表皮生长因子受体;GBM:胶质母细胞瘤;HCQ:羟氯喹;IDH1:异柠檬酸脱氢酶(NADP(+))1/2;MTD:最大耐受剂量;CTC:国家癌症研究所常见毒性标准;MGMT:O-6-甲基鸟嘌呤-DNA 甲基转移酶;OS:总生存期;po qd:口服每日一次;SAE:严重不良事件;TMZ:替莫唑胺;WHO:世界卫生组织。