Hellerstein Marc
University of California at Berkeley, United States.
San Francisco General Hospital, University of California at San Francisco, United States.
Vaccine X. 2020 Dec 11;6:100076. doi: 10.1016/j.jvacx.2020.100076. Epub 2020 Aug 28.
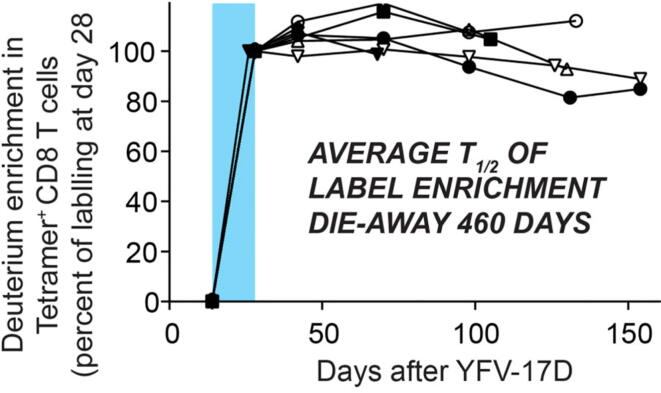
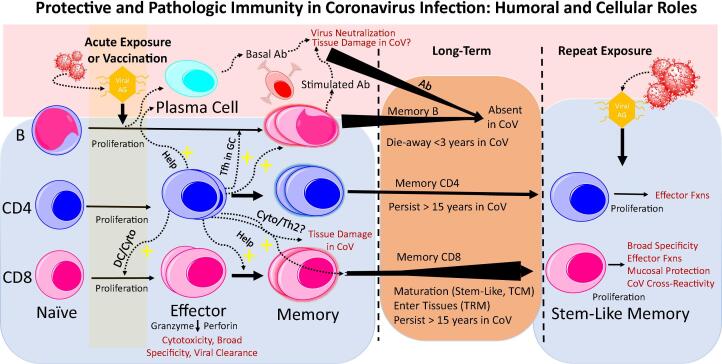
The first SARS-CoV-2 vaccine(s) will likely be licensed based on neutralizing antibodies in Phase 2 trials, but there are significant concerns about using antibody response in coronavirus infections as a sole metric of protective immunity. Antibody response is often a poor marker of prior coronavirus infection, particularly in mild infections, and is shorter-lived than virus-reactive T-cells; strong antibody response correlates with more severe clinical disease while T-cell response is correlated with less severe disease; and antibody-dependent enhancement of pathology and clinical severity has been described. Indeed, it is unclear whether antibody production is protective or pathogenic in coronavirus infections. Early data with SARS-CoV-2 support these findings. Data from coronavirus infections in animals and humans emphasize the generation of a high-quality T cell response in protective immunity. Yellow Fever and smallpox vaccines are excellent benchmarks for primary immune response to viral vaccination and induce long-lived virus-reactive CD8 T-cells, which are present and measurable within 1-4 months of vaccination. Progress in laboratory markers for SARS-CoV2 has been made with identification of epitopes on CD4 and CD8 T-cells in convalescent blood. These are much less dominated by spike protein than in previous coronavirus infections. Although most vaccine candidates are focusing on spike protein as antigen, natural infection by SARS-CoV-2 induces broad epitope coverage, cross-reactive with other betacoronviruses. It will be important to understand the relation between breadth, functionality and durability of T-cell responses and resulting protective immunity. It would be a public health and general trust-in-medicine nightmare - including a boost to anti-vaccine forces - if immune protection wears off or new disease patterns develop among the immunized. Data correlating clinical outcomes with laboratory markers of cell-mediated immunity, not only with antibody response, after SARS-CoV-2 natural infection and vaccines may prove critically valuable if protective immunity fades or if new patterns of disease emerge.
首批严重急性呼吸综合征冠状病毒2(SARS-CoV-2)疫苗可能会基于2期试验中的中和抗体获得许可,但对于将冠状病毒感染中的抗体反应作为保护性免疫的唯一指标存在重大担忧。抗体反应通常不是既往冠状病毒感染的良好标志物,尤其是在轻症感染中,而且其持续时间比病毒反应性T细胞短;强烈的抗体反应与更严重的临床疾病相关,而T细胞反应与较轻的疾病相关;并且已经描述了抗体依赖性的病理和临床严重程度增强。事实上,在冠状病毒感染中,抗体产生是具有保护性还是致病性尚不清楚。SARS-CoV-2的早期数据支持这些发现。来自动物和人类冠状病毒感染的数据强调了在保护性免疫中产生高质量的T细胞反应。黄热病和天花疫苗是病毒疫苗初次免疫反应的优秀基准,可诱导产生长寿的病毒反应性CD8 T细胞,这些细胞在接种疫苗后1至4个月内即可出现并可检测到。通过鉴定康复期血液中CD4和CD8 T细胞上的表位,在SARS-CoV-2的实验室标志物方面取得了进展。与之前的冠状病毒感染相比,这些标志物受刺突蛋白的影响要小得多。尽管大多数候选疫苗都将重点放在刺突蛋白作为抗原上,但SARS-CoV-2的自然感染会诱导广泛的表位覆盖,与其他β冠状病毒具有交叉反应性。了解T细胞反应的广度、功能和持久性与由此产生的保护性免疫之间的关系将很重要。如果免疫保护消失或在接种疫苗者中出现新的疾病模式,这将成为一场公共卫生和公众对医学信任的噩梦——包括增强反疫苗势力。如果保护性免疫减弱或出现新的疾病模式,那么将SARS-CoV-2自然感染和疫苗接种后的临床结果与细胞介导免疫的实验室标志物(而不仅仅是抗体反应)相关联的数据可能会被证明具有至关重要的价值。