Division of Nephrology, Department of Medicine and Surgery, University of Parma, Parma, Italy.
Division of Nephrology, Federal University of São Paulo and Oswaldo Ramos Foundation, São Paulo, Brazil.
J Nephrol. 2021 Aug;34(4):1347-1372. doi: 10.1007/s40620-020-00840-y. Epub 2020 Sep 2.
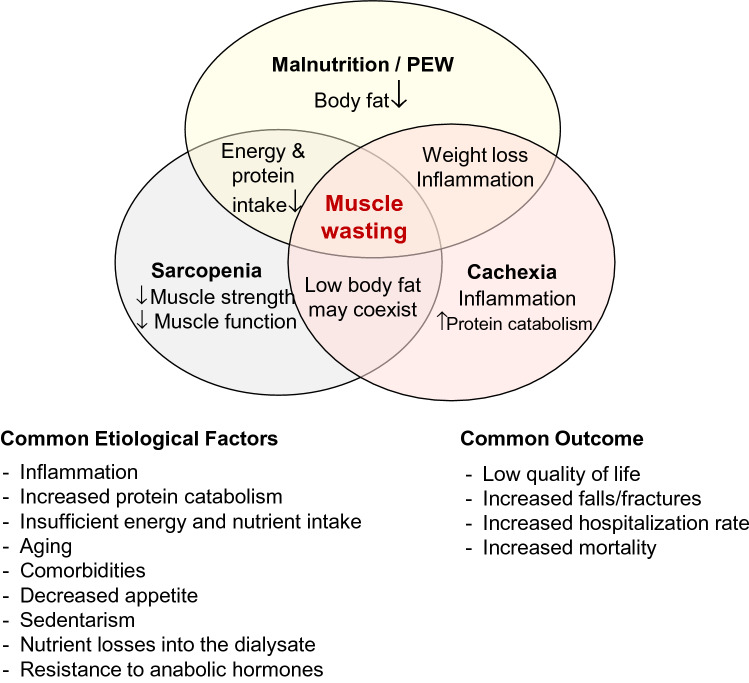
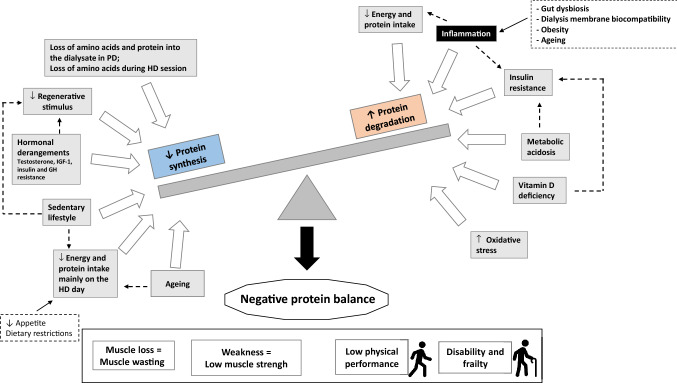
The term sarcopenia was first introduced in 1988 by Irwin Rosenberg to define a condition of muscle loss that occurs in the elderly. Since then, a broader definition comprising not only loss of muscle mass, but also loss of muscle strength and low physical performance due to ageing or other conditions, was developed and published in consensus papers from geriatric societies. Sarcopenia was proposed to be diagnosed based on operational criteria using two components of muscle abnormalities, low muscle mass and low muscle function. This brought awareness of an important nutritional derangement with adverse outcomes for the overall health. In parallel, many studies in patients with chronic kidney disease (CKD) have shown that sarcopenia is a prevalent condition, mainly among patients with end stage kidney disease (ESKD) on hemodialysis (HD). In CKD, sarcopenia is not necessarily age-related as it occurs as a result of the accelerated protein catabolism from the disease and from the dialysis procedure per se combined with low energy and protein intakes. Observational studies showed that sarcopenia and especially low muscle strength is associated with worse clinical outcomes, including worse quality of life (QoL) and higher hospitalization and mortality rates. This review aims to discuss the differences in conceptual definition of sarcopenia in the elderly and in CKD, as well as to describe etiology of sarcopenia, prevalence, outcome, and interventions that attempted to reverse the loss of muscle mass, strength and mobility in CKD and ESKD patients.
肌少症一词于 1988 年由 Irwin Rosenberg 首次提出,用于定义老年人中发生的肌肉丧失状况。此后,由于年龄或其他因素导致的肌肉质量、肌肉力量和身体机能下降的更广泛的定义得到了发展,并在老年医学学会的共识文件中发表。肌少症的诊断基于操作性标准,使用肌肉异常的两个组成部分,即肌肉质量低和肌肉功能低。这引起了人们对重要营养失调的认识,对整体健康产生了不利影响。与此同时,许多慢性肾脏病(CKD)患者的研究表明,肌少症是一种普遍存在的疾病,主要发生在终末期肾脏病(ESKD)接受血液透析(HD)的患者中。在 CKD 中,肌少症不一定与年龄有关,因为它是由疾病和透析本身引起的蛋白质分解加速以及能量和蛋白质摄入不足引起的。观察性研究表明,肌少症,尤其是肌肉力量减弱,与更差的临床结局相关,包括生活质量(QoL)更差、住院率和死亡率更高。本文旨在讨论老年人和 CKD 中肌少症的概念定义差异,并描述肌少症的病因、患病率、结局以及试图逆转 CKD 和 ESKD 患者肌肉质量、力量和活动能力丧失的干预措施。