Department of Urology and Renal Transplantation, Yokohama City University Medical Center, Yokohama, Japan.
Medical Affairs, Janssen Pharmaceutical K.K., Tokyo, Japan.
BMC Urol. 2020 Sep 2;20(1):139. doi: 10.1186/s12894-020-00689-0.
A higher incidence of apalutamide-related skin rash has been observed in Japanese patients with prostate cancer (PC).
This integrated analysis of data of Japanese patients from 2 global Phase 3 studies, SPARTAN ( NCT01946204 ; patients with non-metastatic castration-resistant PC [nmCRPC]) and TITAN ( NCT02489318 ; patients with metastatic castration-sensitive PC [mCSPC]), and the Phase 1 study 56021927PCR1008 ( NCT02162836 ; patients with metastatic CRPC [mCRPC]), assessed clinical risk factors of apalutamide-related skin rash as well as the potential correlation with plasma exposure to apalutamide. Kaplan-Meier method was used for time-to-event analyses. Clinical risk factors for skin rash were assessed using odds ratio.
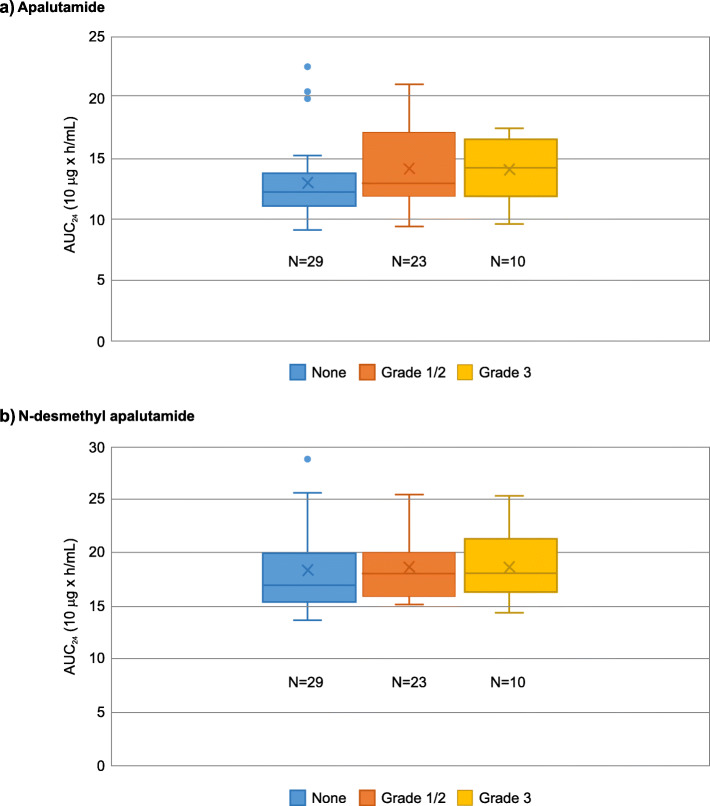
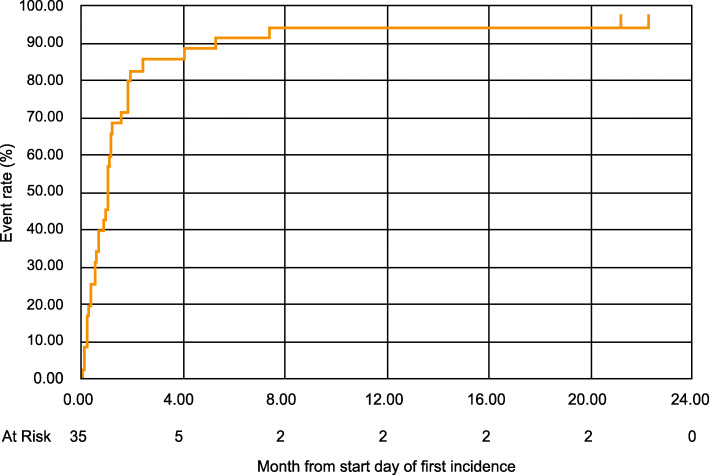
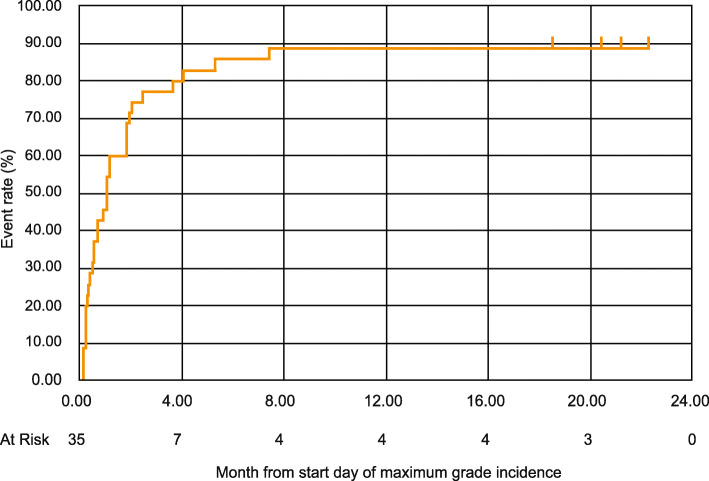
Data from 68 patients (SPARTAN: n = 34, TITAN: n = 28, 56021927PCR1008: n = 6) receiving apalutamide 240 mg orally once-daily were analyzed. Rash (13 [19.1%]) and maculo-papular rash (11 [16.2%]) were the most frequently reported skin rash. All Grade and Grade 3 skin rash occurred in 35 (51.5%) and 10 (14.7%) patients, respectively. Most (85.7%) skin rash occurred within 4 months of apalutamide initiation and resolved in a median time of 1 month following the use of antihistamines, topical or systemic corticosteroids, with/without apalutamide dose interruptions/reductions. Median time-to-remission of first incidence of rash and maximum grade incidence of rash were 1.0 month (IQR: 0.36-1.81) and 1.0 month (IQR: 0.30-2.43), respectively. No significant clinical risk factors for the incidence of skin rash were observed. Areas under the curve (0-24 h) (AUC) at steady-state of plasma apalutamide concentration were numerically slightly higher in patients with skin rash than those without.
No clinical risk factors for rash could be detected. There is a potential correlation between incidence of skin rash and plasma exposure to apalutamide. In general, apalutamide-related skin rash is easily managed, with appropriate treatment with or without dose adjustment.
Retrospective pooled analysis of NCT01946204 , NCT02489318 , and NCT02162836 .
在患有前列腺癌(PC)的日本患者中,阿帕鲁胺相关皮疹的发生率较高。
本研究对来自两项全球 3 期研究(SPARTAN[NCT01946204;非转移性去势抵抗性 PC(nmCRPC)患者]和 TITAN[NCT02489318;转移性去势敏感性 PC(mCSPC)患者])以及 1 项 56021927PCR1008 期研究(NCT02162836;转移性 CRPC(mCRPC)患者)的日本患者数据进行了整合分析,评估了阿帕鲁胺相关皮疹的临床风险因素,并评估了其与阿帕鲁胺血浆暴露的潜在相关性。使用 Kaplan-Meier 法进行生存时间分析。使用比值比评估皮疹的临床风险因素。
对 68 例(SPARTAN:n=34;TITAN:n=28;56021927PCR1008:n=6)接受每日口服 240mg 阿帕鲁胺的患者数据进行了分析。皮疹(13 例[19.1%])和斑丘疹(11 例[16.2%])是最常报告的皮疹。所有等级和 3 级皮疹分别发生在 35 例(51.5%)和 10 例(14.7%)患者中。大多数(85.7%)皮疹发生在阿帕鲁胺治疗开始后 4 个月内,使用抗组胺药、局部或全身皮质类固醇治疗后中位时间为 1 个月,有/无阿帕鲁胺剂量中断/减少。首次皮疹发作的缓解中位时间和最大皮疹等级发作中位时间分别为 1.0 个月(IQR:0.36-1.81)和 1.0 个月(IQR:0.30-2.43)。未观察到皮疹发生率的显著临床风险因素。稳态时血浆阿帕鲁胺浓度的 AUC(0-24 小时)(AUC)数值在皮疹患者中略高于无皮疹患者。
未发现皮疹发生的临床风险因素。皮疹的发生与阿帕鲁胺的血浆暴露可能存在相关性。一般来说,阿帕鲁胺相关皮疹易于管理,适当治疗有/无剂量调整。
NCT01946204、NCT02489318 和 NCT02162836 的回顾性汇总分析。