The Carl and Edyth Lindner Center for Research and Education at The Christ Hospital, Cincinnati, OH, United States of America.
Minneapolis Heart Institute Foundation at Abbott Northwestern Hospital, Minneapolis, MN, United States of America.
Cardiovasc Revasc Med. 2021 Feb;23:86-90. doi: 10.1016/j.carrev.2020.08.019. Epub 2020 Aug 13.
Over the past 20 years, the development of regional ST-elevation myocardial infarction (STEMI) care systems has led to remarkable progress in achieving timely coronary reperfusion with attendant improvement in clinical outcomes, including survival. Despite this progress, contemporary STEMI care does not consistently meet the national guideline-recommended goals, which offers an opportunity for further improvement in STEMI outcomes. The lack of single, comprehensive, national STEMI registry complicates our ability to improve STEMI outcomes in particular for high-risk STEMI subsets such as cardiac arrest (CA) and/or cardiogenic shock (CS).
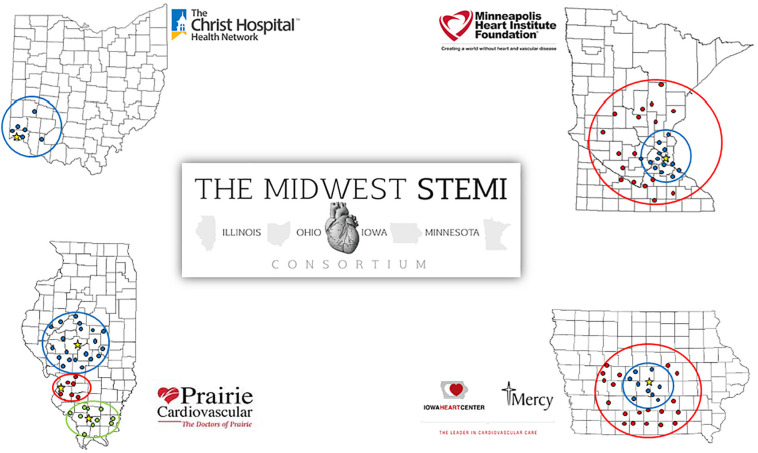
To address this need, the Midwest STEMI Consortium (MSC) was created as a collaboration of 4 large, regional STEMI care systems to provide a comprehensive, multicenter, and prospective STEMI registry without any exclusionary criteria.
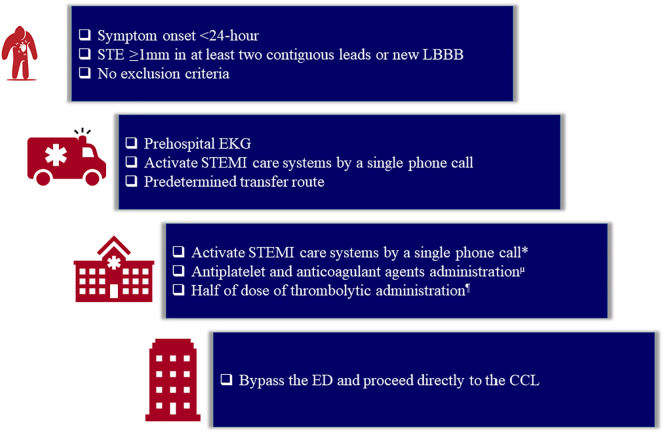
The MSC is a collaboration of 4 large, regional STEMI care systems: Iowa Heart Center in Des Moines, IA; Minneapolis Heart Institute Foundation in Minneapolis, MN; Prairie Heart Institute in Springfield, IL; and The Christ Hospital in Cincinnati, OH. Each has similar standardized STEMI protocol and together include 6 percutaneous coronary intervention (PCI)-capable hospitals and over 100 non-PCI-capable hospitals. Each center had a prospective database that was transferred to a data coordinating center to create the multicenter database. The comprehensive database includes traditional risk factors, cardiovascular history, medications, time to treatment data, detailed angiographic characteristics, and short- and long-term clinical outcomes up to 5-year for myocardial infarction, stroke, and cardiovascular and all-cause mortality. Ten-year mortality rates were assessed by using national death index.
Currently, the comprehensive database (03/2003-01/2020) includes 14,911 consecutive STEMI patients with mean age of 62.3 ± 13.6 years, female gender (29%), and left anterior descending artery as the culprit vessel (34%). High risk features included: Age >75 years (19%), left ventricular ejection fraction <35% (15%), CA (10%), and CS (8%).
This collaboration of 4 large, regional STEMI care systems with broad entry criteria including high-risk STEMI subsets such as CA and/or CS provides a unique platform to conduct clinical research studies to optimize STEMI care.
在过去的 20 年中,区域性 ST 段抬高型心肌梗死(STEMI)治疗系统的发展使得及时进行冠状动脉再灌注治疗取得了显著进展,从而改善了临床结局,包括生存率。尽管取得了这些进展,但当代 STEMI 治疗并未始终符合国家指南推荐的目标,这为进一步改善 STEMI 结局提供了机会。缺乏单一、全面、全国性的 STEMI 登记册使我们难以改善 STEMI 结局,尤其是对于高危 STEMI 亚组,如心搏骤停(CA)和/或心源性休克(CS)。
为满足这一需求,中西部 STEMI 联合会(MSC)成立,由 4 个大型区域性 STEMI 治疗系统合作组成,提供一个全面、多中心、前瞻性的 STEMI 登记册,没有任何排除标准。
MSC 是由 4 个大型区域性 STEMI 治疗系统合作组成:爱荷华州得心中心(Des Moines,IA);明尼苏达州明尼阿波利斯心脏研究所(Minneapolis,MN);春田心脏研究所(Springfield,IL);和辛辛那提基督医院(Cincinnati,OH)。每个系统都有类似的标准化 STEMI 方案,总共包括 6 个经皮冠状动脉介入(PCI)治疗能力的医院和 100 多个非 PCI 治疗能力的医院。每个中心都有一个前瞻性数据库,该数据库被转移到数据协调中心,以创建多中心数据库。全面的数据库包括传统危险因素、心血管病史、药物、治疗时间数据、详细的血管造影特征以及短期和长期临床结局,最长可达 5 年的心肌梗死、卒中和心血管及全因死亡率。通过使用国家死亡索引评估 10 年死亡率。
目前,综合数据库(2003 年 3 月至 2020 年 1 月)包含 14911 例连续 STEMI 患者,平均年龄为 62.3±13.6 岁,女性(29%),罪犯血管为前降支(34%)。高危特征包括:年龄>75 岁(19%)、左心室射血分数<35%(15%)、心搏骤停(10%)和心源性休克(8%)。
该研究由 4 个大型区域性 STEMI 治疗系统合作组成,纳入标准广泛,包括高危 STEMI 亚组,如心搏骤停和/或心源性休克,为优化 STEMI 治疗提供了一个独特的平台,以开展临床研究。