Tan Youwen, Ye Yun, Zhou Xingbei
Medicine (Baltimore). 2020 Sep 4;99(36):e22061. doi: 10.1097/MD.0000000000022061.
Nilotinib is a selective inhibitor of the BCR-ABL tyrosine kinase receptor and is used in the management of chronic myelogenous leukemia (CML). Nilotinib therapy at high doses is associated with elevated serum bilirubin levels. If the serum bilirubin level exceeds 3 times the upper limit of normal, the recommendation is to either adjust nilotinib dosage or temporarily discontinue the treatment. However, it is unclear whether hyperbilirubinemia indicates obvious liver histology damage.
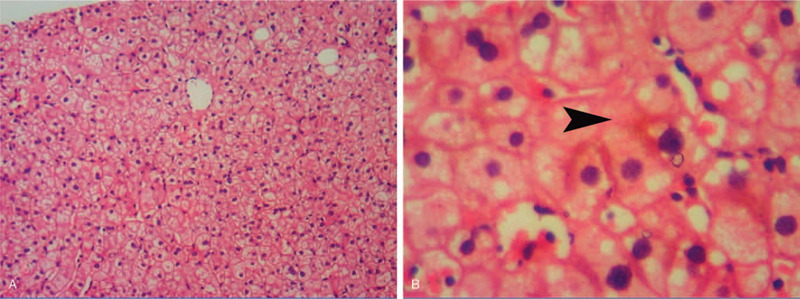
A 24-year-old man with confirmed CML was treated with nilotinib therapy and developed hyperbilirubinemia after the treatment. Although the first remission of the hyperbilirubinemia was achieved after dose adjustment, the hematological parameters deteriorated. Thus, we initiated an antineoplastic therapy (at the standard dose) until complete remission of the CML was achieved. The pathogenic mechanism of hyperbilirubinemia may be related to the inhibition of uridine diphosphate-glucuronosyltransferase (UGT1A1) activity. Liver histological analysis revealed no significant liver damage. In addition, the patient had no family history of hyperbilirubinemia and liver disease.
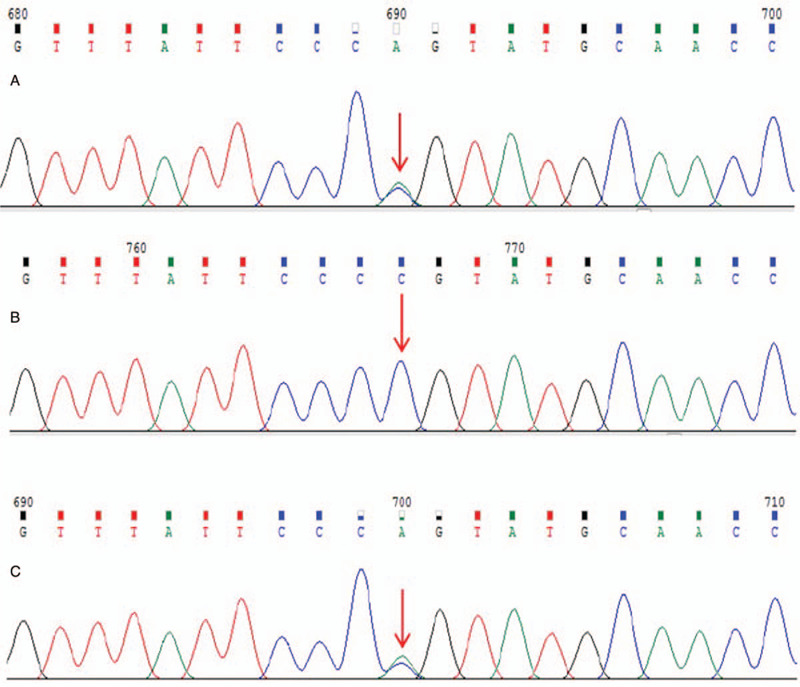
The patient was admitted to our hospital under the diagnosis of hyperbilirubinemia, and histopathology by liver biopsy showed no obvious damage. We also detected a UGT1A1 mutation [ex1 c.686C > A (p.Pro229Gln)] in the patient and his mother.
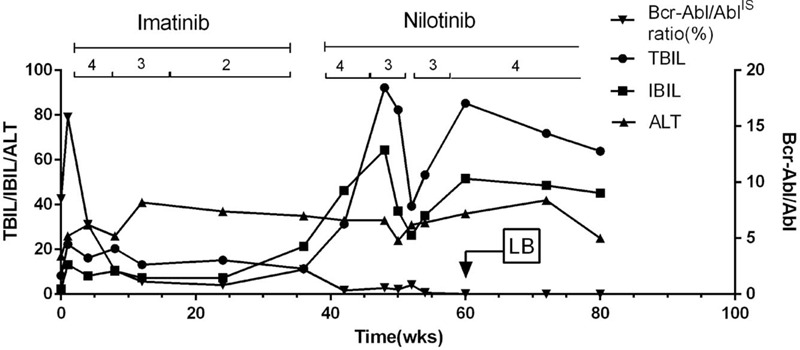
When the nilotinib dose was decreased to 300 mg daily, the total bilirubin (TBIL) level decreased to 30 to 50 μmol/L for 1 month. However, because the Bcr-Abl/Abl ratio did not correspond to the major molecular response (MMR; <0.1%), the nilotinib dose was readjusted to 400 mg daily. One week later, the TBIL and indirect bilirubin levels increased to 89 and 79 μmol/L, respectively. The levels of alanine transaminase and other liver functional indicators were normal.
A Naranjo Adverse Drug Reaction (ADR) Probability Scale score of 13 indicates that hyperbilirubinemia is attributed to ADR caused by nilotinib rather than by drug-induced liver injury.
Although reducing the nilotinib dose can alleviate the occurrence of hyperbilirubinemia, the effect of MMR is also reduced. Treatment of CML without dose adjustment or discontinuation of nilotinib therapy may be more advantageous.
尼洛替尼是一种BCR-ABL酪氨酸激酶受体的选择性抑制剂,用于治疗慢性粒细胞白血病(CML)。高剂量的尼洛替尼治疗与血清胆红素水平升高有关。如果血清胆红素水平超过正常上限的3倍,建议调整尼洛替尼剂量或暂时停止治疗。然而,尚不清楚高胆红素血症是否表明存在明显的肝脏组织学损伤。
一名确诊为CML的24岁男性接受了尼洛替尼治疗,治疗后出现了高胆红素血症。尽管在调整剂量后首次实现了高胆红素血症的缓解,但血液学参数恶化。因此,我们启动了抗肿瘤治疗(标准剂量),直至CML完全缓解。高胆红素血症的发病机制可能与尿苷二磷酸葡萄糖醛酸转移酶(UGT1A1)活性的抑制有关。肝脏组织学分析显示无明显肝损伤。此外,患者无高胆红素血症和肝病家族史。
患者因高胆红素血症入院,肝脏活检的组织病理学检查显示无明显损伤。我们还在患者及其母亲中检测到UGT1A1突变[外显子1 c.686C>A(p.Pro229Gln)]。
当尼洛替尼剂量降至每日300mg时,总胆红素(TBIL)水平在1个月内降至30至50μmol/L。然而,由于Bcr-Abl/Abl比值不符合主要分子反应(MMR;<0.1%),尼洛替尼剂量重新调整为每日400mg。一周后,TBIL和间接胆红素水平分别升至89和79μmol/L。丙氨酸转氨酶和其他肝功能指标水平正常。
Naranjo药物不良反应(ADR)概率量表评分为13,表明高胆红素血症归因于尼洛替尼引起的ADR,而非药物性肝损伤。
虽然降低尼洛替尼剂量可减轻高胆红素血症的发生,但MMR的效果也会降低。在不调整剂量或停用尼洛替尼治疗的情况下治疗CML可能更具优势。