Department of Radiation Oncology, University of Nebraska Medical Center, Omaha.
College of Public Health, Department of Biostatistics, University of Nebraska Medical Center, Omaha.
JAMA Netw Open. 2020 Sep 1;3(9):e2015444. doi: 10.1001/jamanetworkopen.2020.15444.
Immunotherapy has shown significant control of intracranial metastases in patients with melanoma. However, the association of immunotherapy combined with other cancer treatments and overall survival (OS) of patients with brain metastases, regardless of primary tumor site, is unknown.
To explore the association of immunotherapy with OS in patients with cancer and brain metastases who received definitive surgery of the primary site.
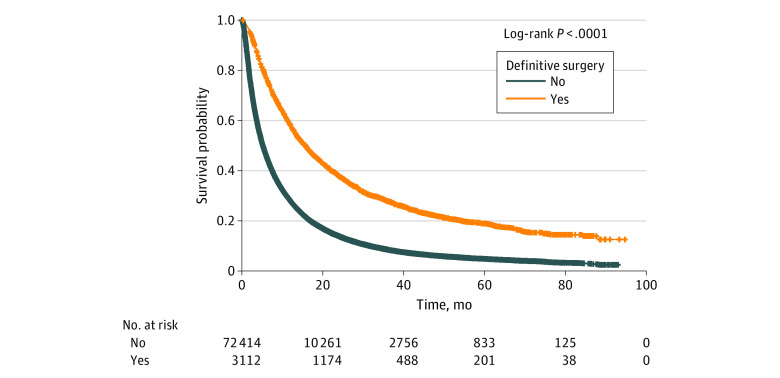
DESIGN, SETTING, AND PARTICIPANTS: This comparative effectiveness study included 3112 adult patients in the National Cancer Database from 2010 to 2016 with non-small cell lung cancer, breast cancer, melanoma, colorectal cancer, or kidney cancer and brain metastases at the time of diagnosis and who received definitive surgery of the primary site. Data analysis was conducted from March to April 2020.
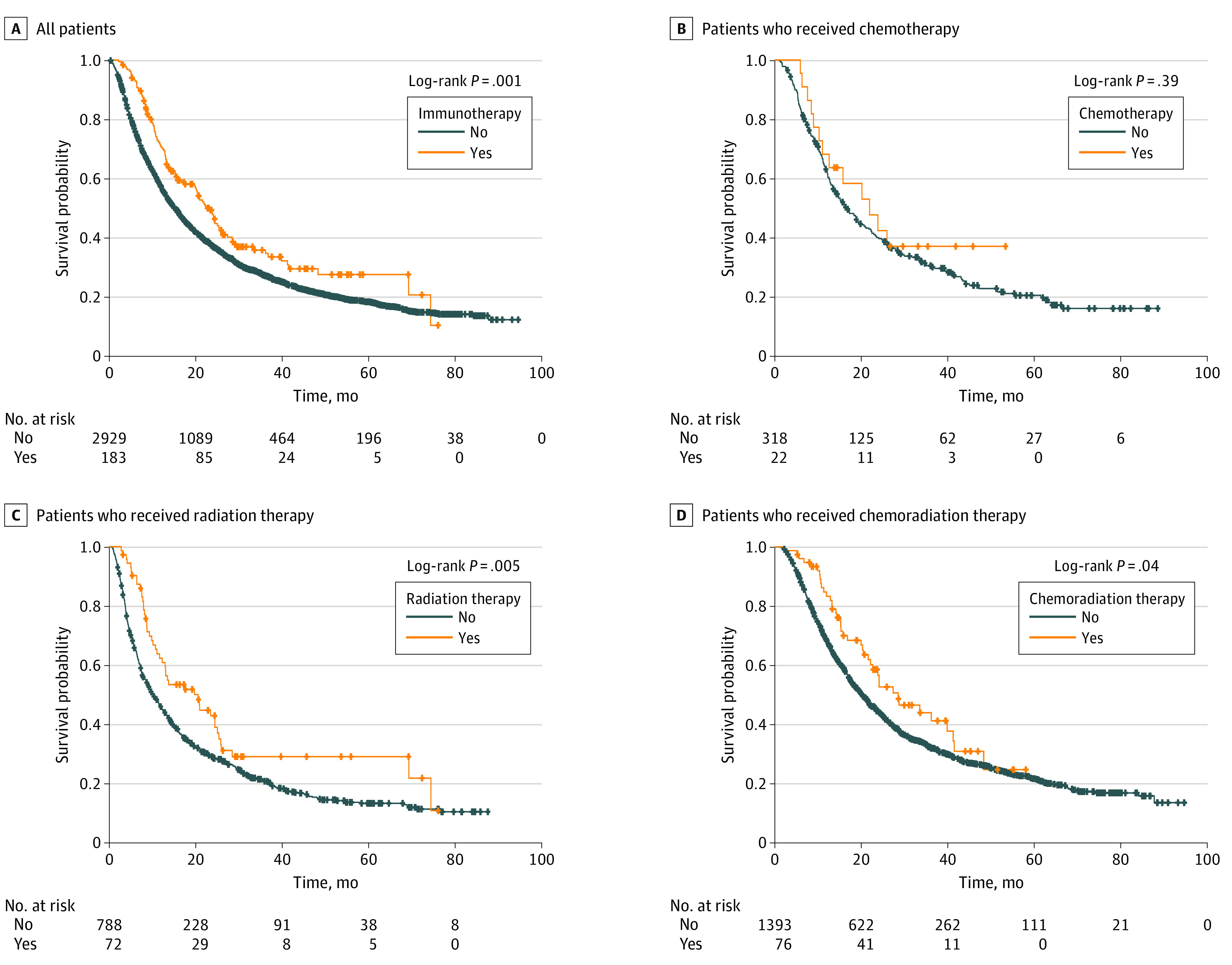
Treatment groups were stratified as follows: (1) any treatment with or without immunotherapy, (2) chemotherapy with or without immunotherapy, (3) radiotherapy (RT) with or without immunotherapy, and (4) chemoradiation with or without immunotherapy.
The association of immunotherapy with OS was assessed with Cox proportional hazards regression, adjusted for age at diagnosis, race, sex, place of living, income, education, treatment facility type, primary tumor type, and year of diagnosis.
Of 3112 patients, 1436 (46.14%) were men, 2714 (87.72%) were White individuals, 257 (8.31%) were Black individuals, and 123 (3.98%) belonged to other racial and ethnic groups. The median (range) age at diagnosis was 61 (19-90) years. Overall, 183 (5.88%) received immunotherapy, 318 (10.22%) received chemotherapy alone, 788 (25.32%) received RT alone, and 1393 (44.76%) received chemoradiation alone; 22 (6.47%) received chemotherapy plus immunotherapy, 72 (8.37%) received RT plus immunotherapy, and 76 (5.17%) received chemoradiation plus immunotherapy. In the multivariable analysis, patients who received immunotherapy had significantly improved OS compared with no immunotherapy (hazard ratio, 0.62; 95% CI, 0.51-0.76; P < .001). Treatment with RT plus immunotherapy was associated with significantly improved OS compared with RT alone (hazard ratio, 0.59; 95% CI, 0.42-0.84; P = .003). Chemotherapy plus immunotherapy or chemoradiation plus immunotherapy were not associated with improved OS in the multivariable analysis.
In this study, the addition of immunotherapy to RT was associated with improved OS compared with radiotherapy alone in patients with brain metastases who received definitive surgery of the primary tumor site.
免疫疗法已显示出对黑色素瘤患者颅内转移的显著控制作用。然而,联合其他癌症治疗的免疫疗法与脑转移患者的总生存期(OS)之间的关联,无论原发肿瘤部位如何,目前尚不清楚。
探讨免疫疗法与接受原发部位确定性手术的脑转移癌症患者 OS 的关系。
设计、地点和参与者:这项比较有效性研究纳入了 2010 年至 2016 年期间,来自国家癌症数据库的 3112 名年龄在 19 岁至 90 岁之间的非小细胞肺癌、乳腺癌、黑色素瘤、结直肠癌或肾癌脑转移患者,他们在诊断时就已经发生了脑转移,并接受了原发部位的确定性手术。数据分析于 2020 年 3 月至 4 月进行。
将治疗组分层如下:(1)任何治疗联合或不联合免疫疗法,(2)化疗联合或不联合免疫疗法,(3)放疗(RT)联合或不联合免疫疗法,以及(4)放化疗联合或不联合免疫疗法。
使用 Cox 比例风险回归评估免疫疗法与 OS 的关联,调整了年龄、种族、性别、居住地、收入、教育、治疗设施类型、原发肿瘤类型和诊断年份。
3112 名患者中,1436 名(46.14%)为男性,2714 名(87.72%)为白人,257 名(8.31%)为黑人,123 名(3.98%)属于其他种族和民族群体。中位(范围)诊断年龄为 61(19-90)岁。总体而言,183 名(5.88%)患者接受了免疫疗法,318 名(10.22%)患者单独接受了化疗,788 名(25.32%)患者单独接受了 RT,1393 名(44.76%)患者单独接受了放化疗;22 名(6.47%)患者接受了化疗联合免疫疗法,72 名(8.37%)患者接受了 RT 联合免疫疗法,76 名(5.17%)患者接受了放化疗联合免疫疗法。多变量分析显示,与未接受免疫治疗的患者相比,接受免疫治疗的患者 OS 显著改善(风险比,0.62;95%CI,0.51-0.76;P<0.001)。与单纯 RT 相比,RT 联合免疫治疗与 OS 显著改善相关(风险比,0.59;95%CI,0.42-0.84;P=0.003)。在多变量分析中,化疗联合免疫疗法或放化疗联合免疫疗法与 OS 改善无关。
在这项研究中,与单纯放疗相比,在接受原发肿瘤部位确定性手术的脑转移患者中,RT 联合免疫疗法可显著改善 OS。