Mesguich Charles, Hulin Cyrille, Latrabe Valerie, Asselineau Julien, Bordenave Laurence, Perez Paul, Hindie Elif, Marit Gerald
Nuclear Medicine Department, Centre Hospitalier Universitaire de Bordeaux, Pessac, France.
INSERM U1035, Université de Bordeaux, Bordeaux, France.
JMIR Res Protoc. 2020 Sep 10;9(9):e17850. doi: 10.2196/17850.
The International Myeloma Working Group recommends the use of 18-fluorodeoxyglucose (FDG) positron emission tomography/computed tomography (PET/CT) for treatment response evaluation, as it is superior to magnetic resonance imaging (MRI). However, at initial staging, the sensitivity of FDG-PET remains inferior to that of MRI. Therefore, there is a need for an imaging technique that could have a sensitivity equal to that of MRI at diagnosis and could serve to evaluate therapy. 18F-choline has shown increased sensitivity when compared with 18-FDG, with about 75% more lesions detected in patients with relapsed or progressive multiple myeloma (MM).
Our primary objective is to prospectively compare the detection rate of bone lesions by 18F-choline PET/CT (FCH-PET) and FDG-PET in newly diagnosed MM. Our secondary objectives are to assess the accuracy of both PET modalities for the detection of bone lesions and the diagnosis of diffuse disease, to assess the detection rate of extramedullary lesions.
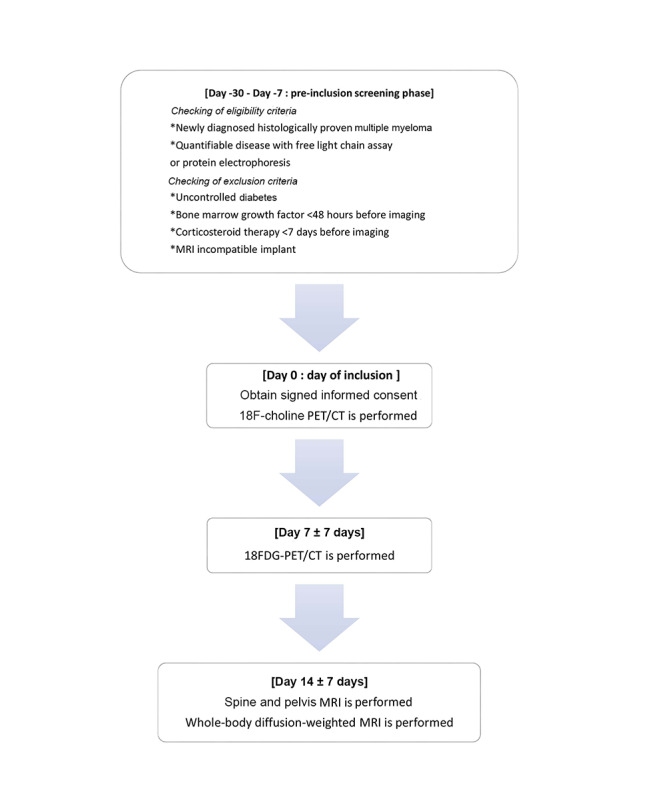
We will prospectively include 30 patients in a paired comparative accuracy study. Patients with de novo MM will undergo FCH-PET, FDG-PET, and whole-body MRI (WB-MRI) within a 3-week period. WB-MRI will be composed of conventional sequences on the spine and pelvis and of whole-body diffusion axial sequences. The following 6 skeletal areas will be defined: skull, sternum/costal grid, spine, pelvis, superior limbs, and inferior limbs. The number of focal lesions, their respective localization, and intensity of uptake will be retrieved for each skeletal area. Readings will be performed blinded from other imaging techniques. The reference standard will be WB-MRI. Focal lesions present on PET/CT but not on WB-MRI will require a decision made with a consensus of experts based on clinical and imaging data. The number of bone lesions and number of extramedullary lesions will be compared using the Wilcoxon test. The accuracy of FCH-PET and FDG-PET will be compared using the McNemar test.
The study started in September 2019, and enrollment is ongoing. As of June 2020, 8 participants have been included. Data collection is expected to be completed in June 2021, and the results are expected to be available in December 2021.
This study will assess if FCH-PET is superior to FDG-PET for the evaluation of MM tumor burden. This will pave the way for future prospective evaluations of the prognostic value of 18-FCH for treatment response evaluation in MM patients. Additionally, this work may provide new perspectives for better assessment of the risk of smoldering MM progressing to MM.
ClinicalTrials.gov NCT03891914; https://clinicaltrials.gov/ct2/show/NCT03891914.
INTERNATIONAL REGISTERED REPORT IDENTIFIER (IRRID): DERR1-10.2196/17850.
国际骨髓瘤工作组建议使用18-氟脱氧葡萄糖(FDG)正电子发射断层扫描/计算机断层扫描(PET/CT)进行治疗反应评估,因为它优于磁共振成像(MRI)。然而,在初始分期时,FDG-PET的敏感性仍低于MRI。因此,需要一种在诊断时敏感性与MRI相当且可用于评估治疗的成像技术。与18-FDG相比,18F-胆碱在复发或进展性多发性骨髓瘤(MM)患者中显示出更高的敏感性,检测到的病变多出约75%。
我们的主要目的是前瞻性比较18F-胆碱PET/CT(FCH-PET)和FDG-PET在新诊断MM中骨病变的检出率。我们的次要目的是评估两种PET模式检测骨病变和诊断弥漫性疾病的准确性,评估髓外病变的检出率。
我们将前瞻性纳入30例患者进行配对比较准确性研究。初发MM患者将在3周内接受FCH-PET、FDG-PET和全身MRI(WB-MRI)检查。WB-MRI将由脊柱和骨盆的常规序列以及全身扩散轴向序列组成。将定义以下6个骨骼区域:颅骨、胸骨/肋格栅、脊柱、骨盆、上肢和下肢。将获取每个骨骼区域的局灶性病变数量、其各自的定位和摄取强度。阅读将在不了解其他成像技术的情况下进行。参考标准将是WB-MRI。PET/CT上存在但WB-MRI上不存在的局灶性病变将需要根据临床和成像数据由专家达成共识做出决定。将使用Wilcoxon检验比较骨病变数量和髓外病变数量。将使用McNemar检验比较FCH-PET和FDG-PET的准确性。
该研究于2019年9月开始,入组正在进行中。截至2020年6月,已纳入8名参与者。数据收集预计于2021年6月完成,结果预计于2021年12月可得。
本研究将评估FCH-PET在评估MM肿瘤负荷方面是否优于FDG-PET。这将为未来前瞻性评估18-FCH对MM患者治疗反应评估的预后价值铺平道路。此外,这项工作可能为更好地评估冒烟型MM进展为MM的风险提供新的视角。
ClinicalTrials.gov NCT03891914;https://clinicaltrials.gov/ct2/show/NCT03891914。
国际注册报告识别码(IRRID):DERR1-10.2 / 196 / 17850。