From the Departments of Epidemiology (M.J.K., H.H.H.A., D.V., S.J.v.d.L., P.Y., M.W.V., N.A., C.M.v.D., M.A.I.), Radiology and Nuclear Medicine (H.H.H.A., P.Y., A.v.d.L., M.W.V.), and Clinical Genetics (H.H.H.A.), Erasmus MC University Medical Center, Rotterdam, the Netherlands; Stroke Research Group, Department of Clinical Neurosciences (D.L., M.T., J.L., D.J.T., H.S.M.), University of Cambridge, UK; Department of Neurology (J.R.J.R., C.L.S., J.J.H., A.S.B., C.D., S. Seshadri), Boston University School of Medicine; The Framingham Heart Study (J.R.J.R., C.L.S., J.J.H., A.S.B., S. Seshadri), MA; Department of Biostatistics (A.V.S.), University of Michigan, Ann Arbor; Icelandic Heart Association (A.V.S., S. Sigurdsson, V.G.), Kopavogur, Iceland; Brown Foundation Institute of Molecular Medicine, McGovern Medical School (M.F.), and Human Genetics Center, School of Public Health (M.F.), University of Texas Health Science Center at Houston; Clinical Division of Neurogeriatrics, Department of Neurology (E.H., L.P., R.S.), Institute for Medical Informatics, Statistics and Documentation (E.H.), and Gottfried Schatz Research Center, Department of Molecular Biology and Biochemistry (Y.S., H.S.), Medical University of Graz, Austria; Center of Cerebrovascular Diseases, Department of Neurology (J.L.), West China Hospital, Sichuan University, Chengdu; Stroke Research Centre, Queen Square Institute of Neurology (I.C.H., D.W., H.H., D.J.W.), University College London, UK; Department of Neurosurgery (I.C.H.), Klinikum rechts der Isar, University of Munich, Germany; Centre for Cognitive Ageing and Cognitive Epidemiology, Psychology (M.L., D.C.M.L., M.E.B., I.J.D., J.M.W.), and Centre for Clinical Brain Sciences, Edinburgh Imaging, UK Dementia Research Institute (M.E.B., J.M.W.), University of Edinburgh, UK; Department of Internal Medicine, Section of Gerontology and Geriatrics (S.T.), Department of Cardiology (S.T., J.v.d.G., J.W.J.), Section of Molecular Epidemiology, Biomedical Data Sciences (E.B.v.d.A., M.B., P.E.S.), Leiden Computational Biology Center, Biomedical Data Sciences (E.B.v.d.A.), Department of Radiology (J.v.d.G.), and Einthoven Laboratory for Experimental Vascular Medicine (J.W.J.), Leiden University Medical Center, the Netherlands; Department of Neurology (A.-K.G., N.S.R.), Massachusetts General Hospital, Harvard Medical School, Boston; Memory Aging and Cognition Center (S.H., C.C.), National University Health System, Singapore; Department of Pharmacology (S.H., C.C.) and Saw Swee Hock School of Public Health (S.H.), National University of Singapore and National University Health System, Singapore; Pattern Recognition & Bioinformatics (E.B.v.d.A.), Delft University of Technology, the Netherlands; Department of Biostatistics (S.L., J.J.H., Q.Y., A.S.B.), Boston University School of Public Health, MA; Department of Radiology (C.R.J., K.K.), Mayo Clinic, Rochester, MN; Glenn Biggs Institute for Alzheimer's & Neurodegenerative Diseases (C.L.S., S. Seshadri), UT Health San Antonio, TX; Department of Medicine, Division of Geriatrics (B.G.W., T.H.M), and Memory Impairment and Neurodegenerative Dementia (MIND) Center (T.H.M.), University of Mississippi Medical Center, Jackson; Singapore Eye Research Institute (C.Y.C., J.Y.K., T.Y.W.); Department of Neuroradiology (Z.M., J.M.W.), NHS Lothian, Edinburgh; Institute of Cardiovascular and Medical Sciences (D.J.S.), College of Medical, Veterinary and Life Sciences, University of Glasgow, UK; Division of Cerebrovascular Neurology (R.F.G.), Johns Hopkins University, Baltimore, MD; Department of Neuroradiology (A.D.M.), Atkinson Morley Neurosciences Centre, St George's NHS Foundation Trust, London, UK; Department of Neurology (C.D.), University of California at Davis; Nuffield Department of Population Health (C.M.v.D.), University of Oxford, UK; Laboratory of Epidemiology and Population Sciences (L.J.L.), National Institute on Aging, Baltimore, MD; and Faculty of Medicine (V.G.), University of Iceland, Reykjavik, Iceland.
Data used in preparation of this article were obtained from the Alzheimer's Disease Neuroimaging Initiative (ADNI) database (adni.loni.usc.edu). As such, the investigators within the ADNI contributed to the design and implementation of ADNI and/or provided data but did not participate in analysis or writing of this report. A complete listing of ADNI investigators can be found in the coinvestigators list at links.lww.com/WNL/B222.
Neurology. 2020 Dec 15;95(24):e3331-e3343. doi: 10.1212/WNL.0000000000010852. Epub 2020 Sep 10.
To identify common genetic variants associated with the presence of brain microbleeds (BMBs).
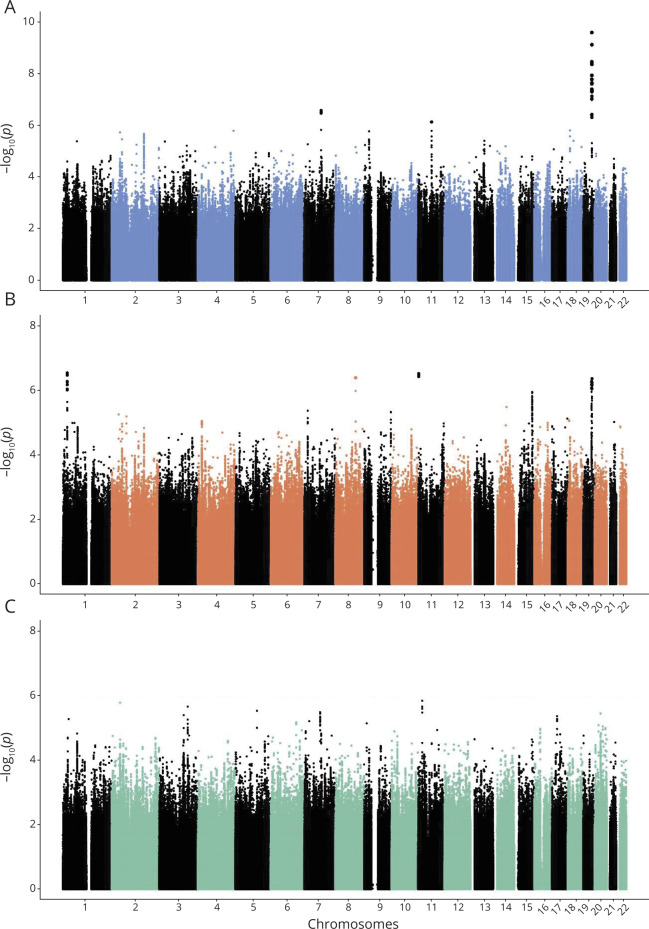
We performed genome-wide association studies in 11 population-based cohort studies and 3 case-control or case-only stroke cohorts. Genotypes were imputed to the Haplotype Reference Consortium or 1000 Genomes reference panel. BMBs were rated on susceptibility-weighted or T2*-weighted gradient echo MRI sequences, and further classified as lobar or mixed (including strictly deep and infratentorial, possibly with lobar BMB). In a subset, we assessed the effects of ε2 and ε4 alleles on BMB counts. We also related previously identified cerebral small vessel disease variants to BMBs.
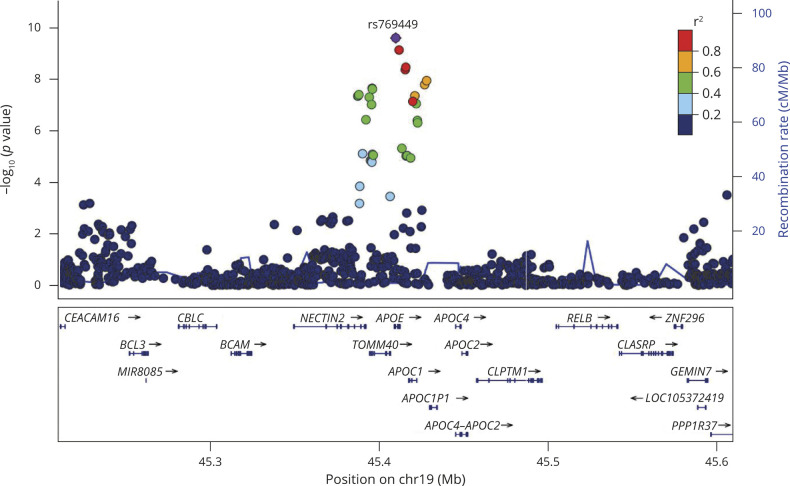
BMBs were detected in 3,556 of the 25,862 participants, of which 2,179 were strictly lobar and 1,293 mixed. One locus in the region reached genome-wide significance for its association with BMB (lead rs769449; odds ratio [OR] [95% confidence interval (CI)] 1.33 [1.21-1.45]; = 2.5 × 10). ε4 alleles were associated with strictly lobar (OR [95% CI] 1.34 [1.19-1.50]; = 1.0 × 10) but not with mixed BMB counts (OR [95% CI] 1.04 [0.86-1.25]; = 0.68). ε2 alleles did not show associations with BMB counts. Variants previously related to deep intracerebral hemorrhage and lacunar stroke, and a risk score of cerebral white matter hyperintensity variants, were associated with BMB.
Genetic variants in the region are associated with the presence of BMB, most likely due to the ε4 allele count related to a higher number of strictly lobar BMBs. Genetic predisposition to small vessel disease confers risk of BMB, indicating genetic overlap with other cerebral small vessel disease markers.
确定与脑微出血(BMB)存在相关的常见遗传变异。
我们在 11 项基于人群的队列研究和 3 项病例对照或病例-only 卒中队列中进行了全基因组关联研究。基因型被推断到 Haplotype Reference Consortium 或 1000 Genomes 参考面板。BMB 是在敏感加权或 T2*-加权梯度回波 MRI 序列上进行评分的,并进一步分类为脑叶或混合性(包括严格的脑叶和幕下,可能伴有脑叶 BMB)。在一个亚组中,我们评估了 ε2 和 ε4 等位基因对 BMB 计数的影响。我们还将先前确定的脑小血管疾病变异与 BMB 相关联。
在 25862 名参与者中,3556 名检测到 BMB,其中 2179 名是严格的脑叶性,1293 名是混合性。在 区域的一个位点因与 BMB 相关而达到全基因组显著水平(主要 rs769449;比值比[OR] [95%置信区间(CI)] 1.33 [1.21-1.45]; = 2.5 × 10)。ε4 等位基因与严格的脑叶性(OR [95% CI] 1.34 [1.19-1.50]; = 1.0 × 10)但与混合性 BMB 计数无关(OR [95% CI] 1.04 [0.86-1.25]; = 0.68)。ε2 等位基因与 BMB 计数无关联。先前与深部脑内出血和腔隙性卒中和脑白质高信号变异风险评分相关的变异与 BMB 相关。
区域中的遗传变异与 BMB 的存在相关,最有可能是由于与更多严格的脑叶性 BMB 相关的 ε4 等位基因计数所致。小血管疾病的遗传易感性赋予了 BMB 的风险,表明与其他脑小血管疾病标志物存在遗传重叠。