Kinoshita Masaki, Inoue Katsuji, Higashi Haruhiko, Akazawa Yusuke, Sasaki Yasuhiro, Fujii Akira, Uetani Teruyoshi, Inaba Shinji, Aono Jun, Nagai Takayuki, Nishimura Kazuhisa, Ikeda Shuntaro, Yamaguchi Osamu
Department of Cardiology, Pulmonology, Hypertension and Nephrology, Ehime University Graduate School of Medicine, Shitsukawa, Toon, Ehime, 791-0295, Japan.
ESC Heart Fail. 2020 Dec;7(6):3810-3820. doi: 10.1002/ehf2.12968. Epub 2020 Sep 13.
Traditional criteria for heart transplantation by cardiopulmonary exercise testing (CPX) include peak oxygen uptake (VO ) < 14 mL/kg/min. Reaching a sufficient exercise load is challenging for patients with refractory heart failure (HF) because of their exercise intolerance. Recently, a substantial impact of right ventricular (RV) dysfunction was highlighted on urgent heart transplantation and mortality. This study aims to investigate the impact of RV contractile reserve, assessed by low-load exercise stress echocardiography (ESE), on exercise intolerance defined as peak VO < 14 mL/kg/min, in patients with HF.
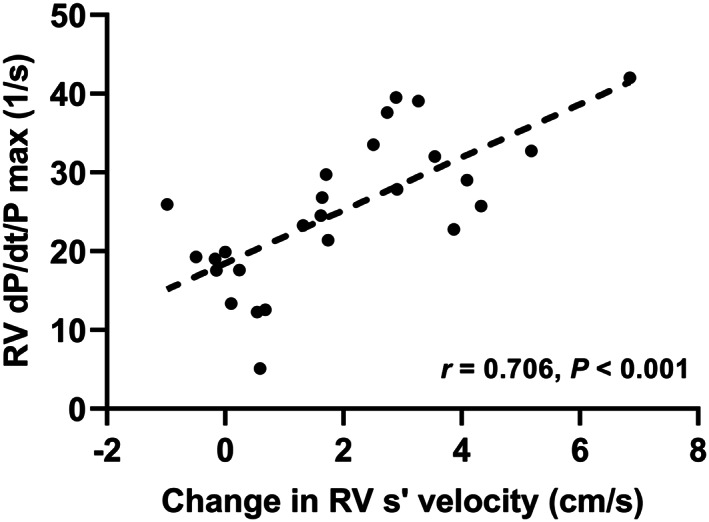
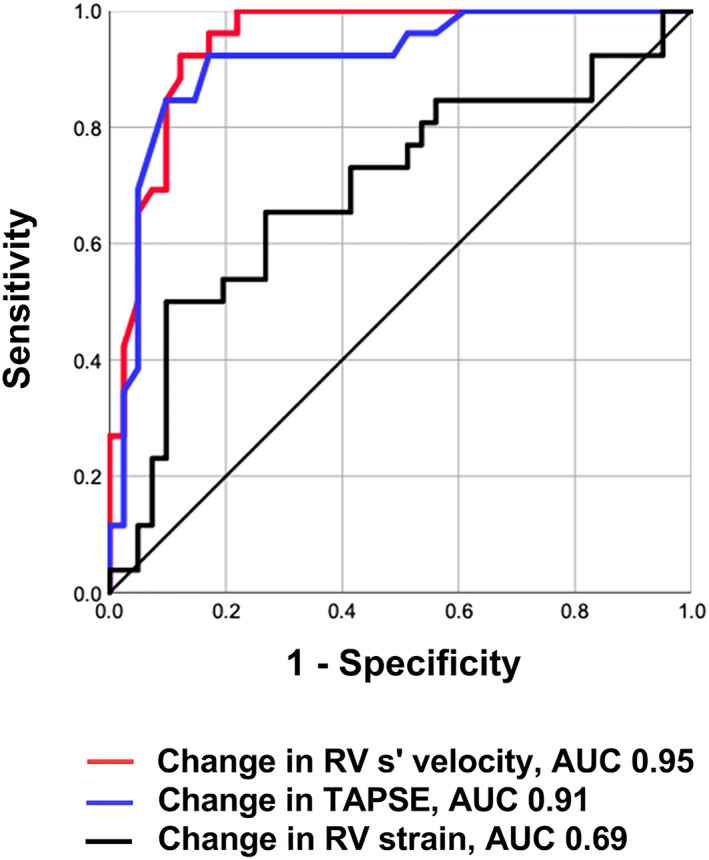
We prospectively examined 67 consecutive patients hospitalized for HF who underwent ESE and CPX under a stabilized HF condition. Although low-load ESE was defined as 25 W load exercise, an increment in RV systolic (s') velocity was regarded as the preservation of RV contractile reserve. All patients completed low-load ESE. During low-load ESE, the variation in RV s' velocity significantly correlated with peak VO (r = 0.787, P < 0.001). The change in RV s' velocity during low-load ESE accurately identified patients with peak VO < 14 mL/kg/min (area under the curve, 0.95; sensitivity, 92%; specificity, 85%). The intraclass correlation coefficient for intra-observer and inter-observer agreement for the change in RV s' velocity was 0.96 (95% confidence interval, 0.88-0.99, P < 0.001) and 0.86 (95% confidence interval, 0.64-0.95, P < 0.001), respectively. The RV-to-pulmonary circulation (PC) coupling, which was assessed by the slope of the relationship between RV s' velocity and pulmonary artery systolic pressure at rest and low-load exercise, was worse in the low-peak VO group (<14 mL/kg/min) than the preserved-peak VO group (≥14 mL/kg/min).
The change in RV s' velocity during low-load ESE could estimate the exercise capacity in HF patients. The assessments of RV contractile reserve and RV-to-PC coupling could be clinically beneficial to distinguish high-risk HF patients.
通过心肺运动试验(CPX)进行心脏移植的传统标准包括峰值摄氧量(VO₂)<14 ml/kg/min。对于难治性心力衰竭(HF)患者而言,由于其运动不耐受,达到足够的运动负荷具有挑战性。最近,右心室(RV)功能障碍对紧急心脏移植和死亡率的重大影响得到了强调。本研究旨在探讨通过低负荷运动应激超声心动图(ESE)评估的RV收缩储备对定义为峰值VO₂<14 ml/kg/min的运动不耐受的HF患者的影响。
我们前瞻性地检查了67例因HF住院的连续患者,这些患者在HF病情稳定的情况下接受了ESE和CPX检查。尽管低负荷ESE定义为25 W负荷运动,但RV收缩期(s')速度的增加被视为RV收缩储备的保留。所有患者均完成了低负荷ESE。在低负荷ESE期间,RV s'速度的变化与峰值VO₂显著相关(r = 0.787,P < 0.001)。低负荷ESE期间RV s'速度的变化准确识别出峰值VO₂<14 ml/kg/min的患者(曲线下面积,0.95;敏感性,92%;特异性,85%)。RV s'速度变化的观察者内和观察者间一致性的组内相关系数分别为0.96(95%置信区间,0.88 - 0.99,P < 0.001)和0.86(95%置信区间,0.64 - 0.95,P < 0.001)。低峰值VO₂组(<14 ml/kg/min)的RV与肺循环(PC)耦合,通过静息和低负荷运动时RV s'速度与肺动脉收缩压之间关系的斜率评估,比保留峰值VO₂组(≥14 ml/kg/min)更差。
低负荷ESE期间RV s'速度的变化可以估计HF患者的运动能力。RV收缩储备和RV与PC耦合的评估在临床上可能有助于区分高危HF患者。