Policy and Management Research Center, School of Health Management, Department of Social Medicine, School of Public Health, Harbin Medical University, No.157 Baojian Road, Nangang District, Harbin, 150086, Heilongjiang, China.
Heilongjiang Provincial Hospital, 82 Zhongshan Road, Xiangfang District, Harbin, 150086, Heilongjiang, China.
Int J Equity Health. 2020 Sep 14;19(1):161. doi: 10.1186/s12939-020-01236-x.
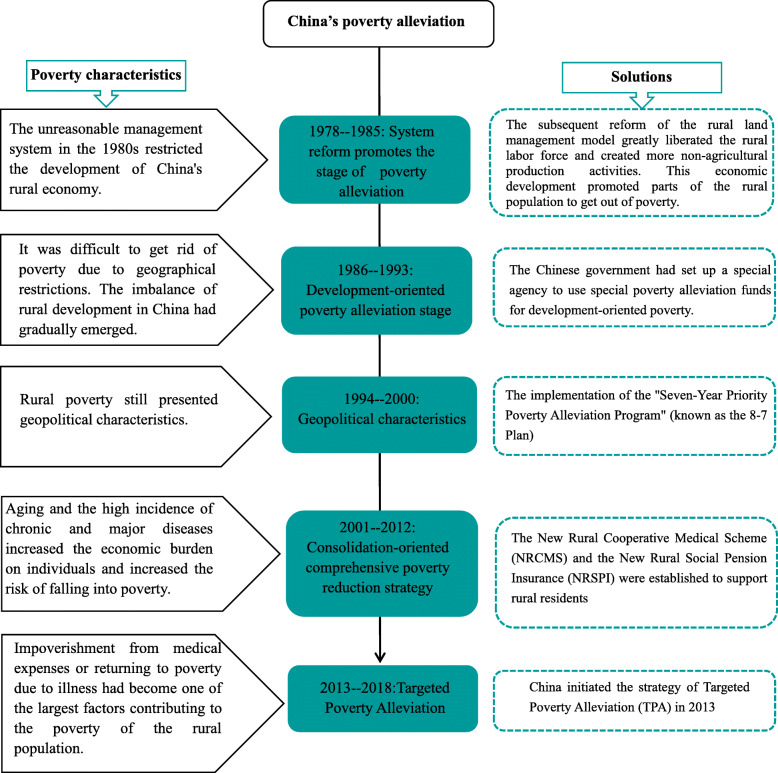
In light of the health poverty alleviation policy, we explore whether the New Rural Cooperative Medical System (NRCMS) has effectively reduced the economic burden of medical expenses on rural middle-aged and elderly people and other impoverished vulnerable groups. The study aims to provide evidence that can be used to improve the medical insurance system.
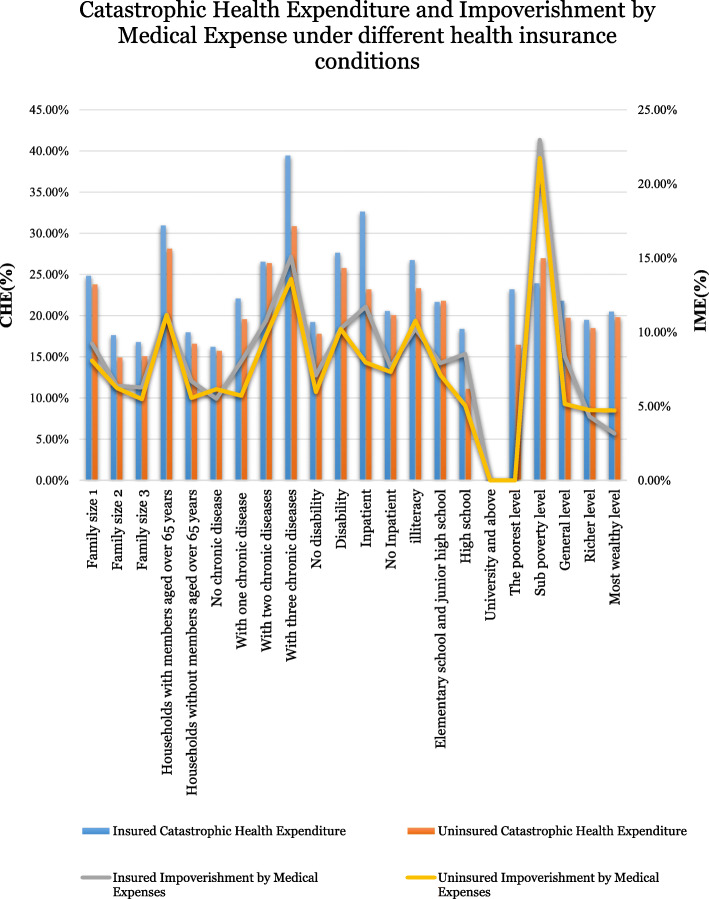
Data were obtained from the 2015 China Health and Retirement Longitudinal Study (CHARLS). The method of calculating the catastrophic health expenditure (CHE) and impoverishment by medical expense (IME) was adopted from the World Health Organization (WHO). The treatment effect model was used to identify the determinants of CHE for rural middle-aged and elderly people.
The incidence of CHE in rural China for middle-aged and elderly people is 21.8%, and the IME is 8.0%. The households that had enrolled in the NRCMS suffered higher CHE (21.9%) and IME (8.0%), than those that had not enrolled (CHE: 20.6% and IME: 7.7%). The NRCMS did not provide sufficient economic protection from CHE for households with three or more chronic diseases, inpatients, or households with members aged over 65 years. Key risk factors for the CHE included education levels, households with inpatients, households with members aged over 65 years, and households with disabilities.
Although the NRCMS has reduced barriers to the usage of household health services by reducing people's out-of-pocket payments, it has not effectively reduced the risk of these households falling into poverty. Our research identifies the characteristics of vulnerable groups that the NRCMS does not provide enough support for, and which puts them at a greater risk of falling into poverty due to health impoverishment.
鉴于健康扶贫政策,我们探讨新型农村合作医疗制度(NRCMS)是否有效减轻了农村中年和老年人群以及其他贫困弱势群体的医疗费用经济负担。本研究旨在为改善医疗保险制度提供证据。
数据来自 2015 年中国健康与退休纵向研究(CHARLS)。采用世界卫生组织(WHO)提出的灾难性卫生支出(CHE)和医疗费用致贫(IME)的计算方法。采用处理效应模型来确定农村中年和老年人 CHE 的决定因素。
中国农村中年和老年人 CHE 的发生率为 21.8%,IME 为 8.0%。参加 NRCMS 的家庭 CHE(21.9%)和 IME(8.0%)高于未参加的家庭(CHE:20.6%和 IME:7.7%)。NRCMS 并未为患有三种或更多慢性病、住院或 65 岁以上成员的家庭提供足够的 CHE 经济保障。CHE 的关键风险因素包括教育程度、住院家庭、65 岁以上家庭和残疾家庭。
尽管 NRCMS 通过降低人们的自付费用来降低家庭使用卫生服务的障碍,但它并没有有效降低这些家庭陷入贫困的风险。我们的研究确定了 NRCMS 没有足够支持的弱势群体的特征,这使他们因健康贫困而更有可能陷入贫困。