Division of Pediatric Surgery, Department of Surgery, St. Louis Children's Hospital, Washington University in St. Louis School of Medicine, St. Louis, MO, United States of America.
Department of Biomedical Engineering, Washington University in St. Louis, St. Louis, MO, United States of America.
PLoS One. 2020 Sep 15;15(9):e0236964. doi: 10.1371/journal.pone.0236964. eCollection 2020.
Short bowel syndrome (SBS) results from significant loss of small intestinal length. In response to this loss, adaptation occurs, with Epidermal Growth Factor Receptor (EGFR) being a key driver. Besides enhanced enterocyte proliferation, we have revealed that adaptation is associated with angiogenesis. Further, we have found that small bowel resection (SBR) is associated with diminished oxygen delivery and elevated levels of hypoxia-inducible factor 1-alpha (HIF1α).
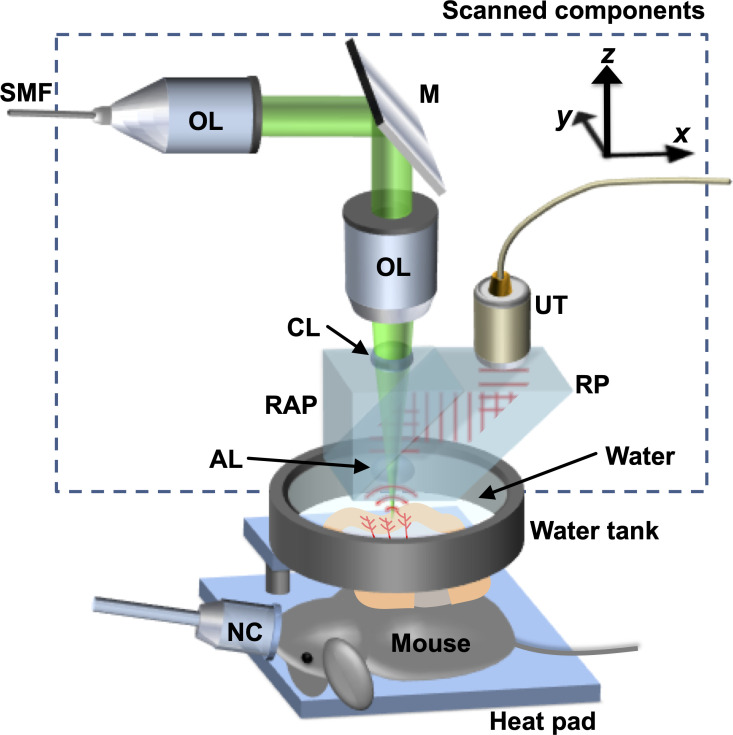
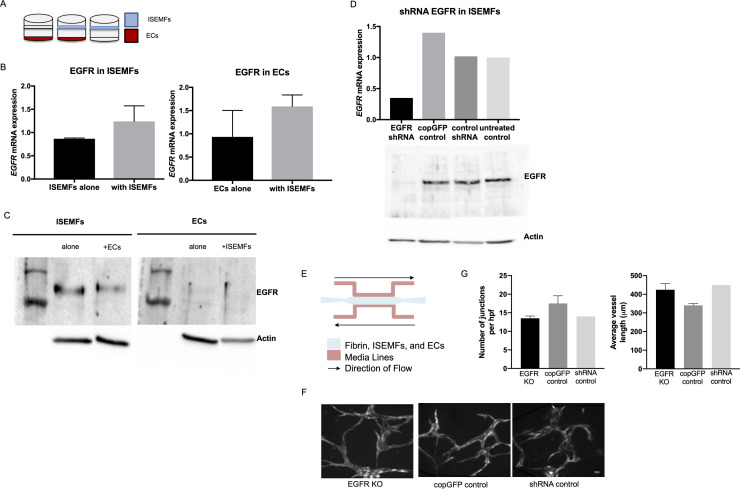
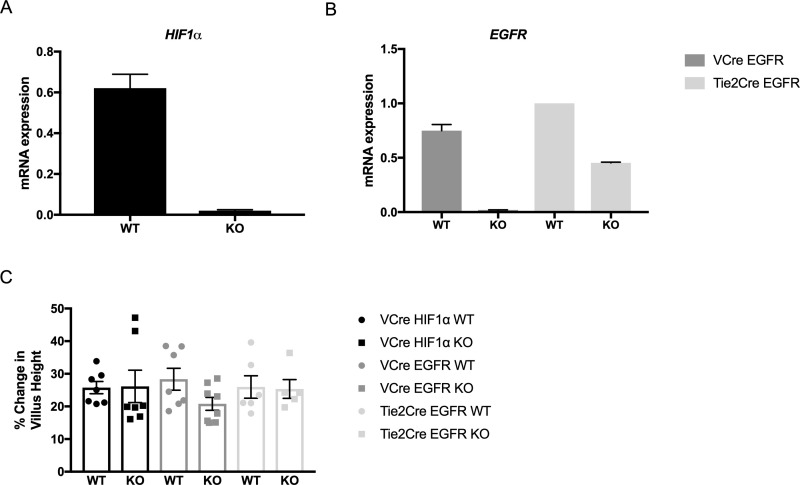
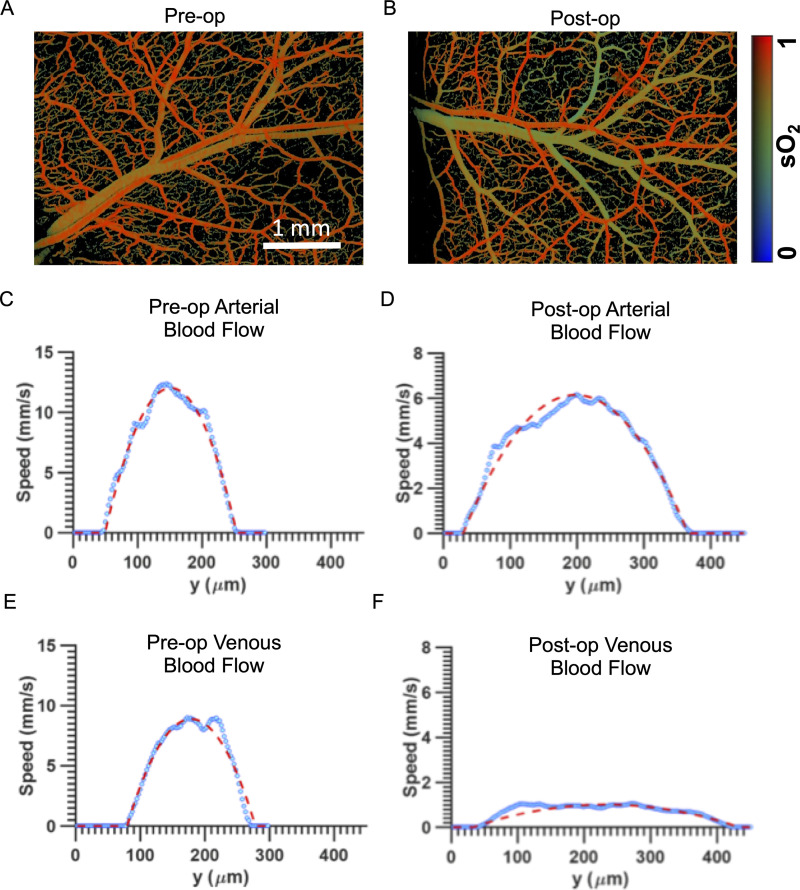
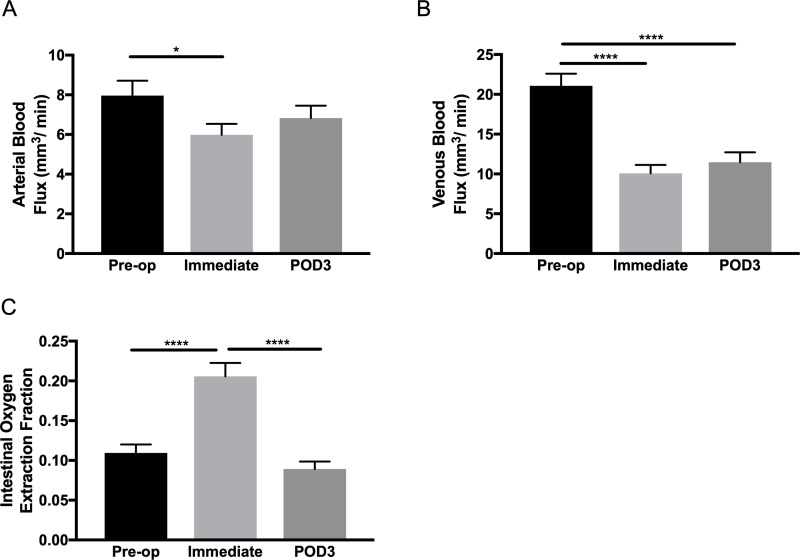
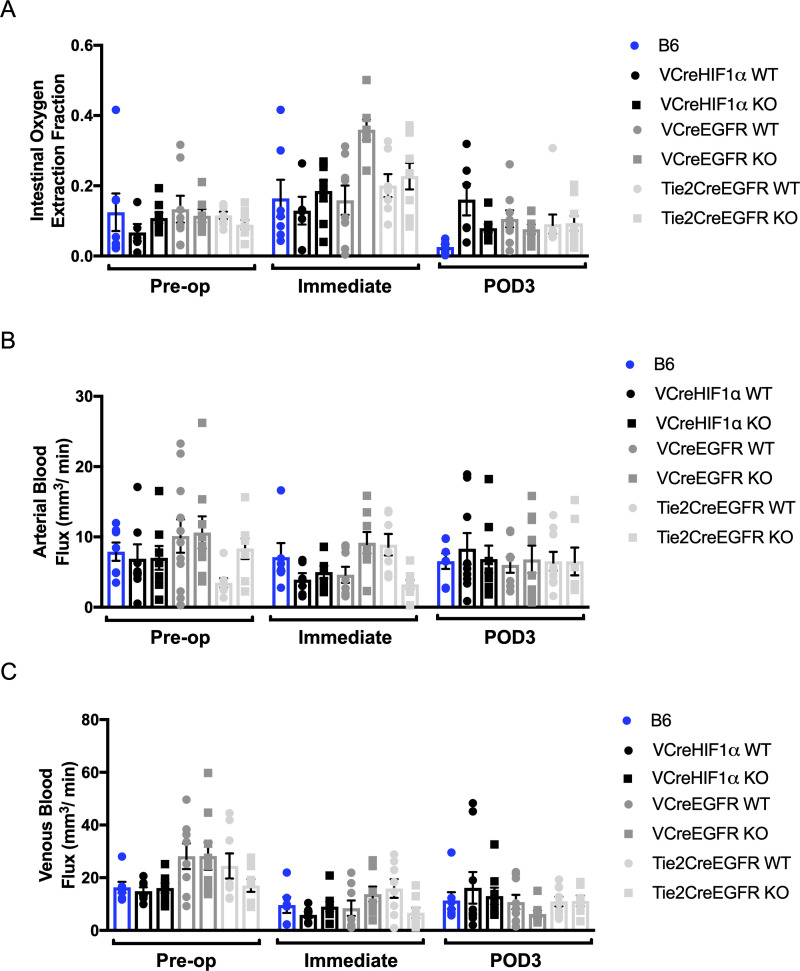
We ablated EGFR in the epithelium and endothelium as well as HIF1α in the epithelium, ostensibly the most hypoxic element. Using these mice, we determined the effects of these genetic manipulations on intestinal blood flow after SBR using photoacoustic microscopy (PAM), intestinal adaptation and angiogenic responses. Then, given that endothelial cells require a stromal support cell for efficient vascularization, we ablated EGFR expression in intestinal subepithelial myofibroblasts (ISEMFs) to determine its effects on angiogenesis in a microfluidic model of human small intestine.
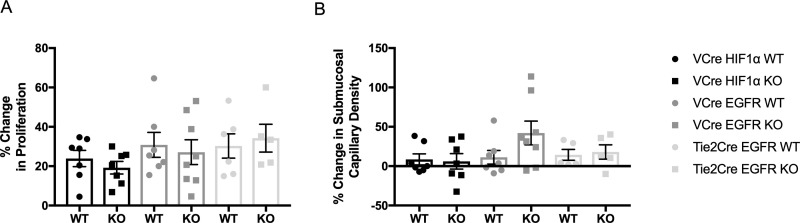
Despite immediate increased demand in oxygen extraction fraction measured by PAM in all mouse lines, were no differences in enterocyte and endothelial cell EGFR knockouts or enterocyte HIF1α knockouts by POD3. Submucosal capillary density was also unchanged by POD7 in all mouse lines. Additionally, EGFR silencing in ISEMFs did not impact vascular network development in a microfluidic device of human small intestine.
Overall, despite the importance of EGFR in facilitating intestinal adaptation after SBR, it had no impact on angiogenesis in three cell types-enterocytes, endothelial cells, and ISEMFs. Epithelial ablation of HIF1α also had no impact on angiogenesis in the setting of SBS.
短肠综合征(SBS)是由于小肠长度显著丧失而引起的。为了应对这种损失,适应性发生了变化,表皮生长因子受体(EGFR)是一个关键驱动因素。除了增强肠细胞增殖外,我们还发现适应性与血管生成有关。此外,我们发现小肠切除术(SBR)与氧输送减少和缺氧诱导因子 1 阿尔法(HIF1α)水平升高有关。
我们在肠上皮细胞和内皮细胞中敲除 EGFR,以及在肠上皮细胞中敲除 HIF1α,这显然是最缺氧的元素。使用这些小鼠,我们通过光声显微镜(PAM)确定了这些基因操作对 SBR 后肠道血流、肠道适应性和血管生成反应的影响。然后,鉴于内皮细胞需要间质支持细胞才能有效地血管化,我们在肠黏膜下肌纤维母细胞(ISEMFs)中敲除 EGFR 表达,以确定其在人小肠微流控模型中的血管生成作用。
尽管在所有小鼠品系中 PAM 立即测量到氧提取分数的增加,但在 POD3 时,肠细胞和内皮细胞 EGFR 敲除或肠细胞 HIF1α 敲除的肠细胞和内皮细胞没有差异。在所有小鼠品系中,POD7 时黏膜下毛细血管密度也没有变化。此外,ISEMFs 中的 EGFR 沉默在人小肠微流控装置中对血管网络发育没有影响。
总的来说,尽管 EGFR 在促进 SBR 后肠道适应性方面很重要,但它对三种细胞类型——肠细胞、内皮细胞和 ISEMFs 的血管生成没有影响。在 SBS 中,上皮细胞中 HIF1α 的缺失也没有影响血管生成。