Duffau Hugues
Department of Neurosurgery, Montpellier University Medical Center, 34295 Montpellier, France.
Institute of Functional Genomics, INSERM U-1191, University of Montpellier, 34298 Montpellier, France.
Cancers (Basel). 2020 Sep 13;12(9):2611. doi: 10.3390/cancers12092611.
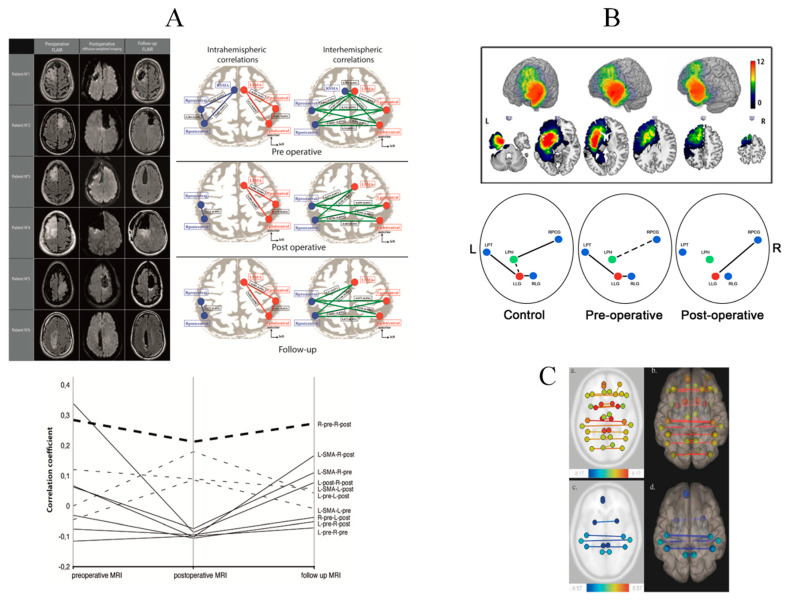
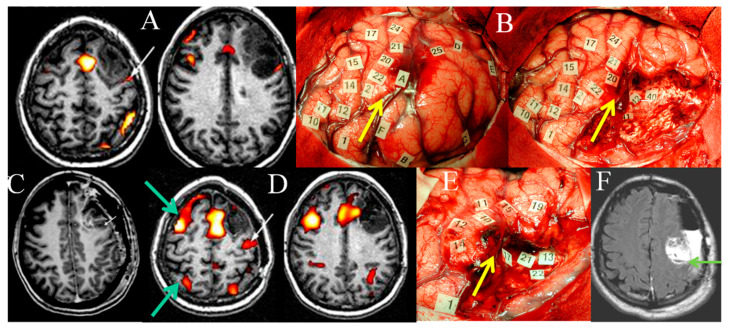
Intraoperative direct electrostimulation mapping (DEM) is currently the gold-standard for glioma surgery, since functional-based resection allows an optimization of the onco-functional balance (increased resection with preserved quality of life). Besides intrasurgical awake mapping of conation, cognition, and behavior, preoperative mapping by means of functional neuroimaging (FNI) and transcranial magnetic stimulation (TMS) has increasingly been utilized for surgical selection and planning. However, because these techniques suffer from several limitations, particularly for direct functional mapping of subcortical white matter pathways, DEM remains crucial to map neural connectivity. On the other hand, non-invasive FNI and TMS can be repeated before and after surgical resection(s), enabling longitudinal investigation of brain reorganization, especially in slow-growing tumors like low-grade gliomas. Indeed, these neoplasms generate neuroplastic phenomena in patients with usually no or only slight neurological deficits at diagnosis, despite gliomas involving the so-called "eloquent" structures. Here, data gained from perioperative FNI/TMS mapping methods are reviewed, in order to decipher mechanisms underpinning functional cerebral reshaping induced by the tumor and its possible relapse, (re)operation(s), and postoperative rehabilitation. Heterogeneous spatiotemporal patterns of rearrangement across patients and in a single patient over time have been evidenced, with structural changes as well as modifications of intra-hemispheric (in the ipsi-lesional and/or contra-lesional hemisphere) and inter-hemispheric functional connectivity. Such various fingerprints of neural reconfiguration were correlated to different levels of cognitive compensation. Serial multimodal studies exploring neuroplasticity might lead to new management strategies based upon multistage therapeutic approaches adapted to the individual profile of functional reallocation.
术中直接电刺激图谱(DEM)目前是胶质瘤手术的金标准,因为基于功能的切除术能够优化肿瘤功能平衡(在保证生活质量的同时增加切除范围)。除了术中对意识、认知和行为进行清醒图谱绘制外,术前通过功能神经影像学(FNI)和经颅磁刺激(TMS)进行的图谱绘制也越来越多地用于手术选择和规划。然而,由于这些技术存在一些局限性,特别是在对皮质下白质通路进行直接功能图谱绘制方面,DEM对于绘制神经连接仍然至关重要。另一方面,非侵入性的FNI和TMS可以在手术切除前后重复进行,从而能够对大脑重组进行纵向研究,尤其是在低级别胶质瘤等生长缓慢的肿瘤中。事实上,尽管胶质瘤累及所谓的“明确功能”结构,但这些肿瘤在诊断时通常没有或只有轻微神经功能缺损的患者中会产生神经可塑性现象。在此,对围手术期FNI/TMS图谱绘制方法所获得的数据进行综述,以解读肿瘤及其可能的复发、再次手术和术后康复所诱导的大脑功能重塑的潜在机制。已经证实了患者之间以及单个患者随时间的异质时空重排模式,包括结构变化以及半球内(同侧病变半球和/或对侧病变半球)和半球间功能连接的改变。这种神经重新配置的各种特征与不同水平的认知补偿相关。探索神经可塑性的系列多模态研究可能会带来基于适应功能重新分配个体特征的多阶段治疗方法的新管理策略。