Department of Radiation Oncology, Tata Memorial Hospital (TMH)/Advanced Centre for Treatment Education & Research in Cancer (ACTREC), Tata Memorial Centre, Homi Bhabha National Institute (HBNI), Kharghar, Mumbai, 410210, India.
Department of Medical Physics, Tata Memorial Hospital (TMH)/Advanced Centre for Treatment Education & Research in Cancer (ACTREC), Tata Memorial Centre, Homi Bhabha National Institute (HBNI), Mumbai, India.
Radiat Oncol. 2020 Sep 16;15(1):218. doi: 10.1186/s13014-020-01666-5.
To compare long-term disease-related outcomes and late radiation morbidity between intensity-modulated radiation therapy (IMRT) and three-dimensional conformal radiotherapy (3D-CRT) in head and neck squamous cell carcinoma (HNSCC) in the setting of a prospective randomized controlled trial.
Previously untreated patients with early to moderately advanced non-metastatic squamous carcinoma of the oropharynx, larynx, or hypopharynx (T1-T3, N0-N2b, M0) planned for comprehensive irradiation of primary site and bilateral neck nodes were randomly assigned to either IMRT or 3D-CRT after written informed consent. Patients were treated with 6MV photons to a total dose of 70Gy/35 fractions over 7 weeks (3D-CRT) or 66Gy/30 fractions over 6 weeks (IMRT). A sample size of 60 patients was estimated to demonstrate 35% absolute difference in the incidence of ≥grade 2 acute xerostomia between the two arms. All time-to-event outcomes were calculated from date of randomization until the defined event using the Kaplan-Meier method.
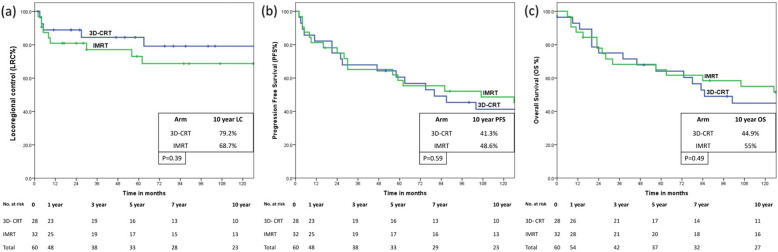
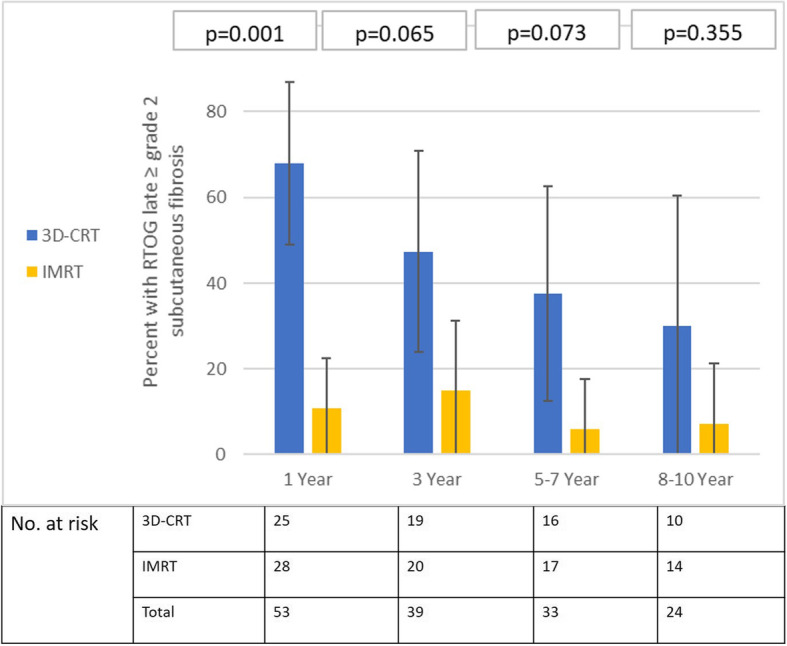
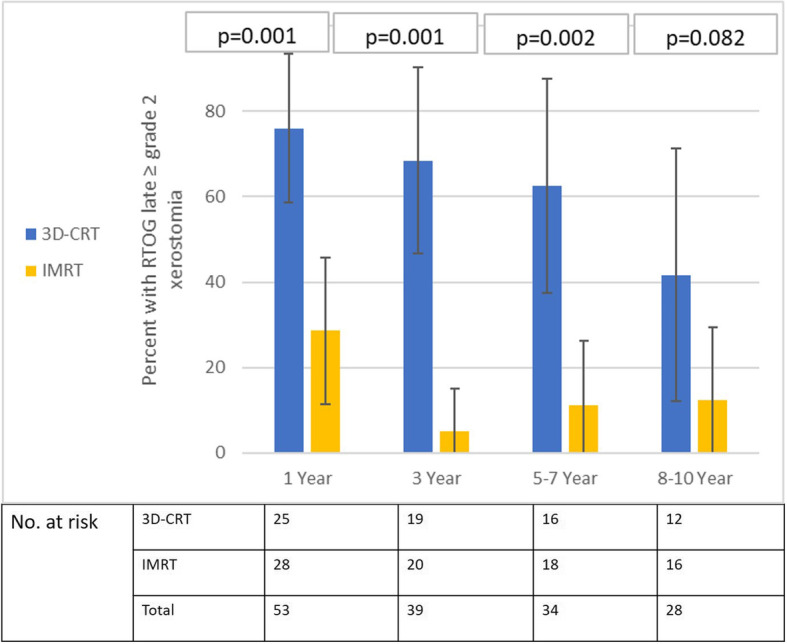
At a median follow-up of 140 months for surviving patients, 10-year Kaplan-Meier estimates of loco-regional control (LRC); progression-free survival (PFS); and overall survival (OS) with 95% confidence interval (95%CI) were 73.6% (95%CI: 61.2-86%); 45.2% (95%CI: 32-58.4%); and 50.3% (95%CI: 37.1-63.5%) respectively. There were no significant differences in 10-year disease-related outcomes between 3D-CRT and IMRT for LRC [79.2% (95%CI: 62.2-96.2%) vs 68.7% (95%CI: 51.1-86.3%), p = 0.39]; PFS [41.3% (95%CI: 22.3-60.3%) vs 48.6% (95%CI: 30.6-66.6%), p = 0.59]; or OS [44.9% (95%CI: 25.7-64.1%) vs 55.0% (95%CI: 37-73%), p = 0.49]. Significantly lesser proportion of patients in the IMRT arm experienced ≥grade 2 late xerostomia and subcutaneous fibrosis at all time-points. However, at longer follow-up, fewer patients remained evaluable for late radiation toxicity reducing statistical power and precision.
IMRT provides a clinically meaningful and sustained reduction in the incidence of moderate to severe xerostomia and subcutaneous fibrosis compared to 3D-CRT without compromising disease-related outcomes in long-term survivors of non-nasopharyngeal HNSCC.
在一项前瞻性随机对照试验中,比较头颈部鳞癌(HNSCC)患者接受调强放疗(IMRT)和三维适形放疗(3D-CRT)的长期疾病相关结局和晚期放射并发症。
入组经病理证实的早期至局部晚期非转移性口咽、喉或下咽鳞癌(T1-T3,N0-N2b,M0)患者,在签署书面知情同意书后,随机分为 IMRT 或 3D-CRT 组,接受原发灶和双侧颈部淋巴结综合照射。患者采用 6MV 光子,70Gy/35 次,7 周(3D-CRT)或 66Gy/30 次,6 周(IMRT)。预计 60 例患者的样本量可证明两组间≥2 级急性口干症的发生率有 35%的绝对差异。所有时间至事件结局均从随机分组日期开始,使用 Kaplan-Meier 法计算至定义事件的时间。
在中位随访 140 个月的生存患者中,10 年 Kaplan-Meier 估计的局部区域控制(LRC);无进展生存期(PFS);总生存期(OS)和 95%置信区间(95%CI)分别为 73.6%(95%CI:61.2-86%);45.2%(95%CI:32-58.4%);50.3%(95%CI:37.1-63.5%)。3D-CRT 和 IMRT 组的 10 年疾病相关结局在 LRC 方面无显著差异[79.2%(95%CI:62.2-96.2%)与 68.7%(95%CI:51.1-86.3%),p=0.39];PFS [41.3%(95%CI:22.3-60.3%)与 48.6%(95%CI:30.6-66.6%),p=0.59];或 OS [44.9%(95%CI:25.7-64.1%)与 55.0%(95%CI:37-73%),p=0.49]。在所有时间点,IMRT 组中发生≥2 级晚期口干症和皮下纤维化的患者比例明显较低。然而,在随访时间较长时,因晚期放射毒性而可评估的患者数量减少,降低了统计效能和精度。
与 3D-CRT 相比,IMRT 可显著降低非鼻咽癌患者头颈部鳞癌的中重度口干症和皮下纤维化的发生率,而不影响长期生存者的疾病相关结局。