From the Division of Cardiovascular Medicine, Lahey Hospital and Medical Center, Burlington, Massachusetts, USA.
Clin Cardiol. 2020 Dec;43(12):1494-1500. doi: 10.1002/clc.23467. Epub 2020 Sep 17.
Left bundle branch block (LBBB) and left ventricular (LV) dyssynchrony likely contribute to progressive systolic dysfunction. The evaluation of newly recognized LBBB includes screening for structural heart abnormalities and coronary artery disease (CAD). In patients whose LV ejection fraction (EF) is preserved during initial testing, the incidence of subsequent cardiomyopathy is not firmly established.
The risk of developing LV systolic dysfunction among LBBB patients with preserved LVEF is high enough to warrant serial imaging.
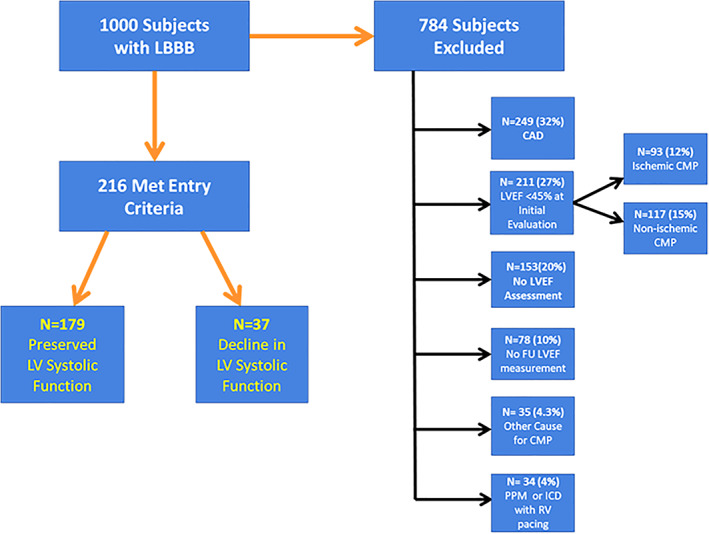
We screened records of 1000 consecutive patients with LBBB from our ECG database and identified subjects with an initially preserved LVEF (≥45%) without clinically relevant CAD or other cause for cardiomyopathy. Baseline imaging, clinical data, and follow-up imaging were recorded to determine the risk of subsequent LV systolic dysfunction (LVEF ≤40%).
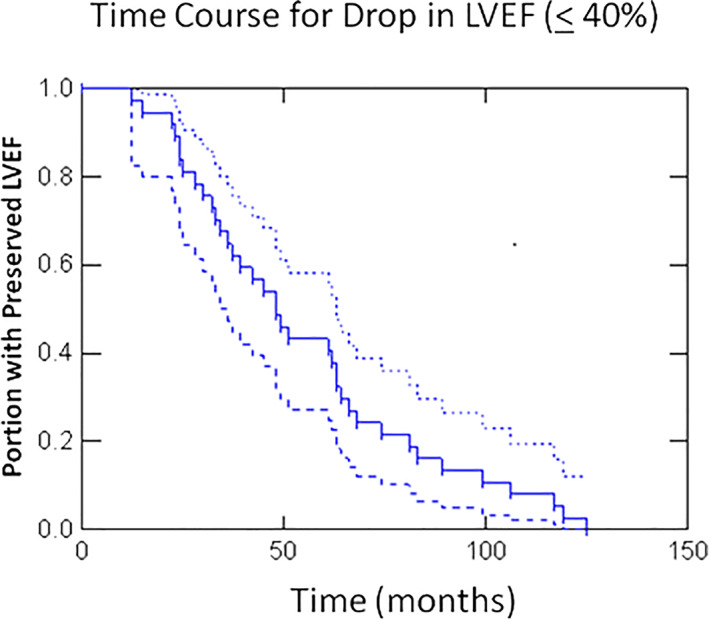
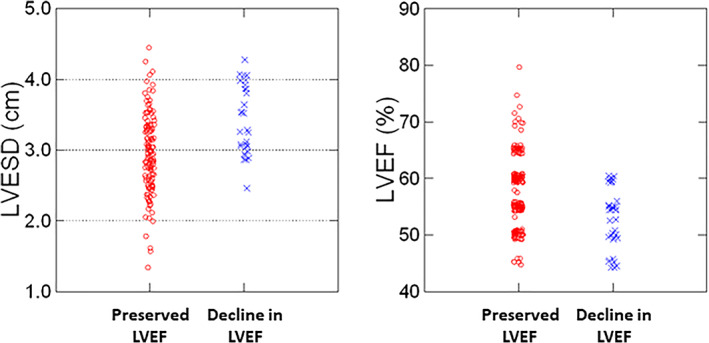
(Data are mean + SD) 784 subjects were excluded, the majority for CAD or depressed LVEF upon initial imaging. Of the remaining 216, 37 (17%) developed a decline in LVEF(≤40%) over a mean follow-up of 55 ± 31 months; 94% of these patients had a baseline LVEF≤60% and LV end systolic diameter (ESD) ≥ 2.9 cm indicating that these measures may be useful to define which patients warrant longitudinal follow-up. The negative predictive value of a LVEF>60% and LVESD <2.9 cm was 98%.
Seventeen percent of patients with LBBB and initial preserved LVEF develop dyssynchrony cardiomyopathy. We believe the risk of developing dyssynchrony cardiomyopathy is high enough to warrant serial assessment of LV systolic function in this high-risk population.
左束支传导阻滞(LBBB)和左心室(LV)不同步可能导致进行性收缩功能障碍。新诊断的 LBBB 的评估包括筛查结构性心脏异常和冠状动脉疾病(CAD)。在最初检查时 LV 射血分数(EF)保留的患者中,随后发生心肌病的发生率尚未确定。
EF 保留的 LBBB 患者发生 LV 收缩功能障碍的风险足够高,需要进行连续成像。
我们从心电图数据库中筛选了 1000 例连续 LBBB 患者的记录,确定了最初 EF(≥45%)保留、无临床相关 CAD 或其他心肌病病因的患者。记录基线影像学、临床数据和随访影像学,以确定随后发生 LV 收缩功能障碍(LVEF ≤40%)的风险。
(数据为平均值 + 标准差)784 例患者被排除在外,大多数是由于 CAD 或初始影像学检查时 LVEF 降低。在剩余的 216 例患者中,37 例(17%)在平均 55 ± 31 个月的随访中 LVEF(≤40%)下降;这些患者中 94%的基线 LVEF≤60%和 LV 收缩末期直径(ESD)≥ 2.9 cm,这表明这些指标可能有助于确定哪些患者需要进行纵向随访。LVEF>60%和 LVESD <2.9 cm 的阴性预测值为 98%。
17%的 LBBB 患者和最初保留的 LVEF 会发生不同步性心肌病。我们认为,发生不同步性心肌病的风险足够高,需要对这一高危人群进行 LV 收缩功能的连续评估。