Division of Experimental Medicine, McGill University Health Center, Montreal, QC, Canada.
Division of Neonatology, McGill University Health Center, Montreal, QC, Canada.
Pediatr Res. 2021 May;89(7):1810-1817. doi: 10.1038/s41390-020-01159-x. Epub 2020 Sep 17.
Extremely preterm infants are often exposed to endotracheal tube continuous positive airway pressure (ETT-CPAP) trials to assess extubation readiness. The effects of ETT-CPAP trial on their diaphragmatic activity (Edi) and breathing variability is unknown.
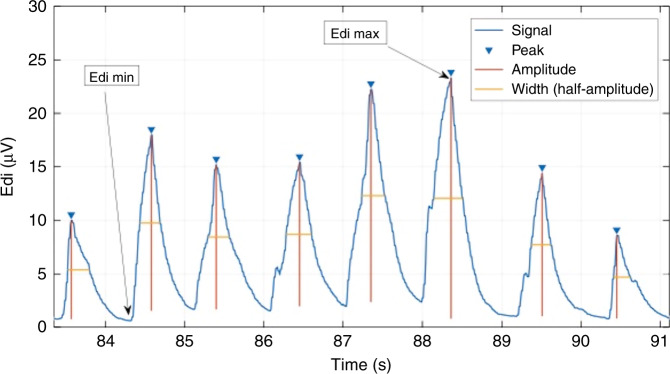
Prospective observational study enrolling infants with birth weight ≤1250 g undergoing their first extubation attempt. Diaphragmatic activity, expressed as the absolute minimum (Edi min) and maximum values (Edi max), area under the Edi signal, and breath-by-breath analyses for breath areas, amplitudes, widths, and neural inspiratory and expiratory times, were analyzed during mechanical ventilation (MV) and ETT-CPAP. Neural breathing variability of each of these parameters was also calculated and compared between MV and ETT-CPAP.
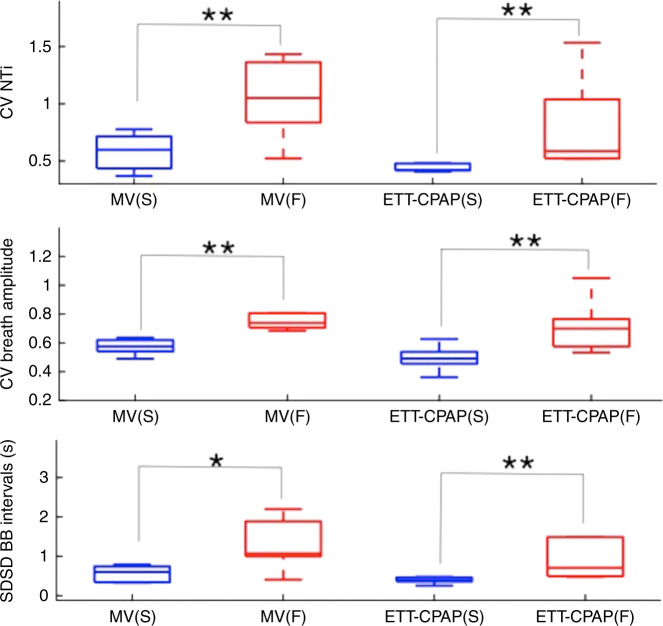
Thirteen infants with median (interquartile range) birth weight of 800 g [610-920] and gestational age of 25.4 weeks [24.4-26.3] were included. Diaphragmatic activity significantly increased during ETT-CPAP when compared to MV:Edi max (44.2 vs. 38.1 μV), breath area (449 vs. 312 μV·s), and amplitude (10.12 vs. 7.46 μV). Neural breathing variability during ETT-CPAP was characterized by increased variability for amplitude and area under the breath, and decreased for breath time and width.
A 5-min ETT-CPAP in extremely preterm infants undergoing extubation imposed significant respiratory load with changes in respiratory variability.
ETT-CPAP trials are often used to assess extubation readiness in extremely preterm infants, but its effects upon their respiratory system are not well known. Diaphragmatic activity analysis demonstrated that these infants are able to mount an important response to a short trial. A 5-min trial imposed a significant respiratory load evidenced by increased diaphragmatic activity and changes in breathing variability. Differences in breathing variability were observed between successful and failed extubations, which should be explored further in extubation readiness investigations. This type of trial cannot be recommended for preterm infants in clinical practice until clear standards and accuracy are established.
极早产儿常需进行气管内持续气道正压通气(ETT-CPAP)试验以评估拔管准备情况。但 ETT-CPAP 试验对其膈肌活动(Edi)和呼吸变异性的影响尚不清楚。
前瞻性观察性研究纳入了接受首次拔管尝试的出生体重≤1250g 的婴儿。在机械通气(MV)和 ETT-CPAP 期间,分析了膈肌活动(以绝对最小值(Edi min)和最大值(Edi max)、Edi 信号下面积以及逐呼吸分析的呼吸幅度、呼吸幅度、呼吸宽度和神经吸气和呼气时间),并计算了这些参数的神经呼吸变异性,并比较了 MV 和 ETT-CPAP 之间的差异。
共纳入 13 名中位(四分位间距)出生体重 800g [610-920]、胎龄 25.4 周 [24.4-26.3]的婴儿。与 MV 相比,ETT-CPAP 时膈肌活动明显增加:Edi max(44.2 vs. 38.1μV)、呼吸幅度(449 vs. 312μV·s)和幅度(10.12 vs. 7.46μV)。ETT-CPAP 时神经呼吸变异性的特征是呼吸幅度和呼吸幅度下面积的变异性增加,呼吸时间和宽度的变异性降低。
对接受拔管的极早产儿进行 5 分钟 ETT-CPAP 试验会显著增加呼吸负荷,并改变呼吸变异性。
ETT-CPAP 试验常用于评估极早产儿的拔管准备情况,但对其呼吸系统的影响尚不清楚。膈肌活动分析表明,这些婴儿能够对短时间的试验做出重要反应。5 分钟的试验会产生显著的呼吸负荷,表现为膈肌活动增加和呼吸变异性改变。在成功和失败的拔管之间观察到呼吸变异性的差异,这需要在拔管准备研究中进一步探讨。在明确标准和准确性之前,这种试验不能在早产儿的临床实践中推荐。