Graves Scott S, Mathes David W, Storb Rainer
Fred Hutchinson Cancer Research Center, 1100 Fairview Avenue N, D1-100, Seattle, WA, U.S.A.
Department of Plastic Surgery, University of Colorado, Aurora, CO.
OBM Transplant. 2019;3(3). doi: 10.21926/obm.transplant.1903080. Epub 2019 Aug 23.
The application of hematopoietic cell transplantation for induction of immune tolerance has been limited by toxicities associated with conditioning regimens and to graft-versus-host disease (GVHD). Decades of animal studies have culminated into sufficient control of these two problems, making immune tolerance a viable alternative to life-long application of immunosuppressive drugs to prevent allograft rejection.
Studies in mice have paved the way for the application of HCT with limited toxicity in large animal models. Resultant studies in the pig, dog, and ultimately the nonhuman primate have led to appropriate methods for achieving nonmyeloablative irradiation protocols, dose, and timing of post-grafting immunosuppressive drugs, monoclonal antibody therapy, and biologicals for costimulatory molecule blockade. The genetics field has been extensively evaluated in appreciation of the ultimate need to obtain organs from MHC-mismatched unrelated donors.
Nonmyeloablative conditioning regimens have been shown to be successful in inducing immune tolerance across all three animal models. Postgrafting immunosuppression is also important in assuring sustained donor hematopoiesis for tolerance. Donor chimerism need not be permanent to establish stable engraftment of donor organs, thereby essentially eliminating the risk of GVHD. Using nonmyeloablative HCT with monoclonal antibody immunosuppression, the kidney has been successfully transplanted in MHC-mismatched nonhuman primates.
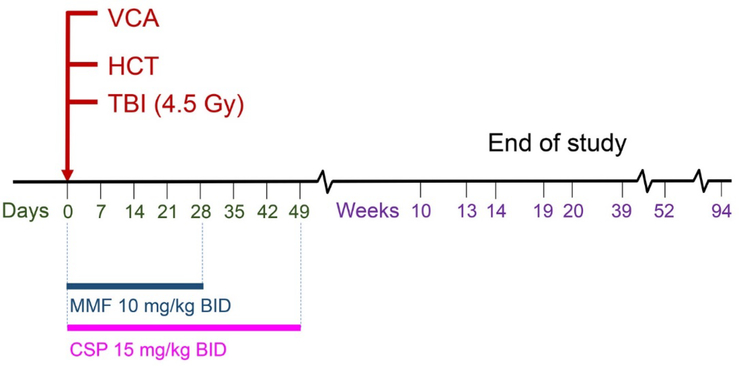
Nonmyeloablative HCT for the establishment of temporary mixed chimerism has led to the establishment of stable tolerance against solid organ allografts in large animal models. The kidney, considered a tolerogenic organ, has been successfully transplanted in the clinic. Other organs such as heart, lung, and vascularized composite allografts (face and hands), remain distant possibilities. Further study in large animal models will be required to improve tolerance against these organs before success can be attained in the clinic.
造血细胞移植诱导免疫耐受的应用受到预处理方案相关毒性以及移植物抗宿主病(GVHD)的限制。数十年的动物研究已充分控制了这两个问题,使免疫耐受成为终身应用免疫抑制药物预防同种异体移植排斥的可行替代方案。
小鼠研究为在大型动物模型中应用低毒性的造血细胞移植铺平了道路。随后在猪、狗以及最终在非人灵长类动物上的研究,得出了实现非清髓性照射方案、移植后免疫抑制药物的剂量和时机、单克隆抗体疗法以及共刺激分子阻断生物制剂的适当方法。鉴于最终需要从MHC不匹配的无关供体获取器官,遗传学领域已得到广泛评估。
非清髓性预处理方案已被证明在所有三种动物模型中成功诱导免疫耐受。移植后免疫抑制对于确保供体造血持续以实现耐受也很重要。供体嵌合体不必永久存在即可建立供体器官的稳定植入,从而基本消除了GVHD的风险。使用非清髓性造血细胞移植和单克隆抗体免疫抑制,肾脏已成功移植到MHC不匹配的非人灵长类动物中。
用于建立临时混合嵌合体的非清髓性造血细胞移植已在大型动物模型中实现了对实体器官同种异体移植的稳定耐受。肾脏被认为是一个具有致耐受性的器官,已在临床上成功移植。心脏、肺和血管化复合异体移植物(面部和手部)等其他器官,在临床上成功实现移植仍遥不可及。在临床上取得成功之前,需要在大型动物模型中进行进一步研究以提高对这些器官的耐受性。