Division of Emergency Medicine, Boston Children's Hospital, Boston, MA.
Pediatr Emerg Care. 2022 Jan 1;38(1):e264-e267. doi: 10.1097/PEC.0000000000002244.
Outcomes of emergency care delivered to children vary by patient-level socioeconomic factors and by emergency department (ED) characteristics, including pediatric volume. How these factors intersect in emergency care-seeking patterns among children is not well understood. The objective of this study was to characterize national associations of neighborhood income and insurance type of children with the characteristics of the EDs from which they receive care.
We conducted a cross-sectional study of ED visits by children from 2014 to 2017 using the Nationwide Emergency Department Sample. We determined the associations of neighborhood income and patient insurance type with the proportions of visits to EDs by pediatric volume category, both unadjusted and adjusted for patient-level factors including urban-rural status of residence.
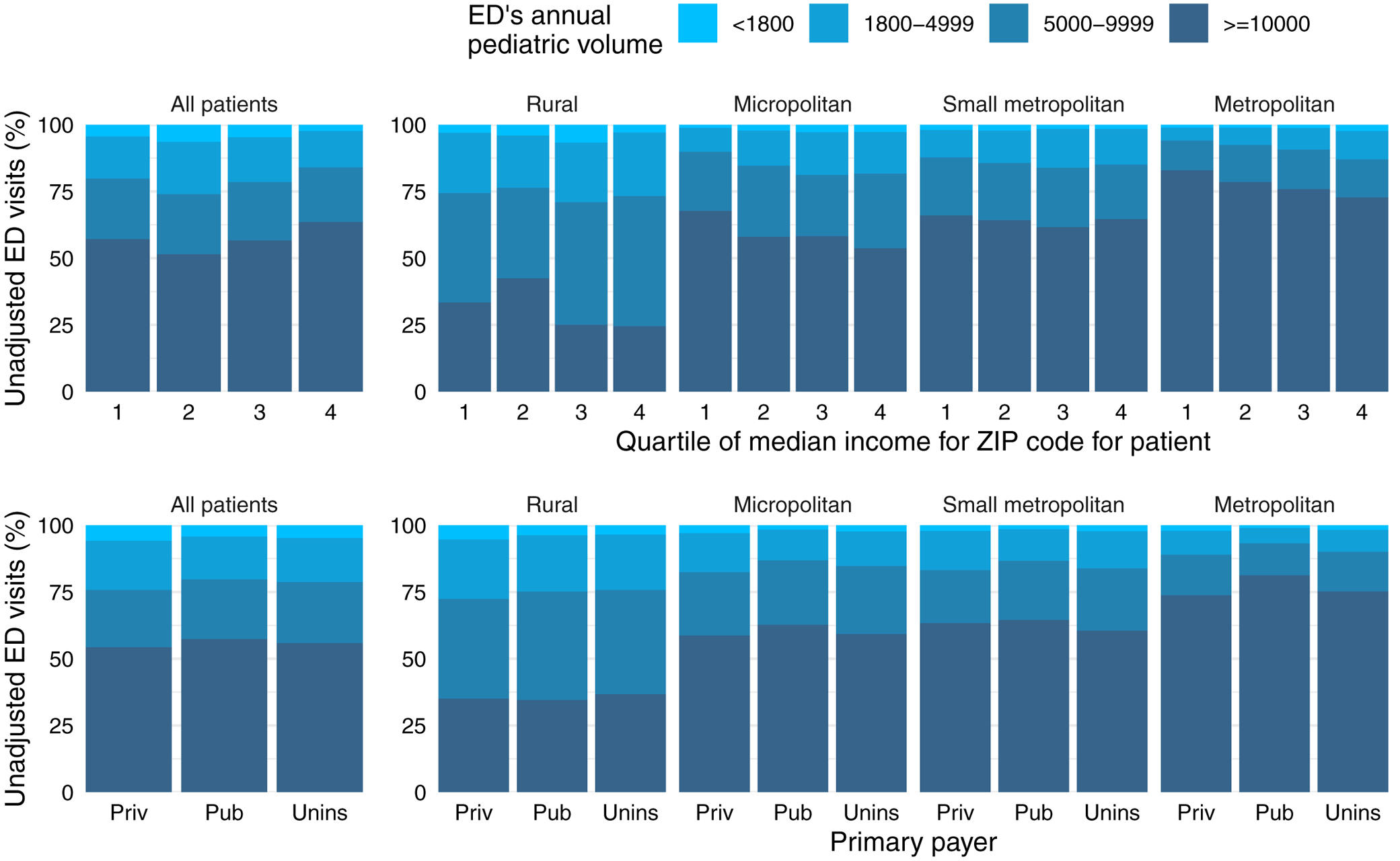
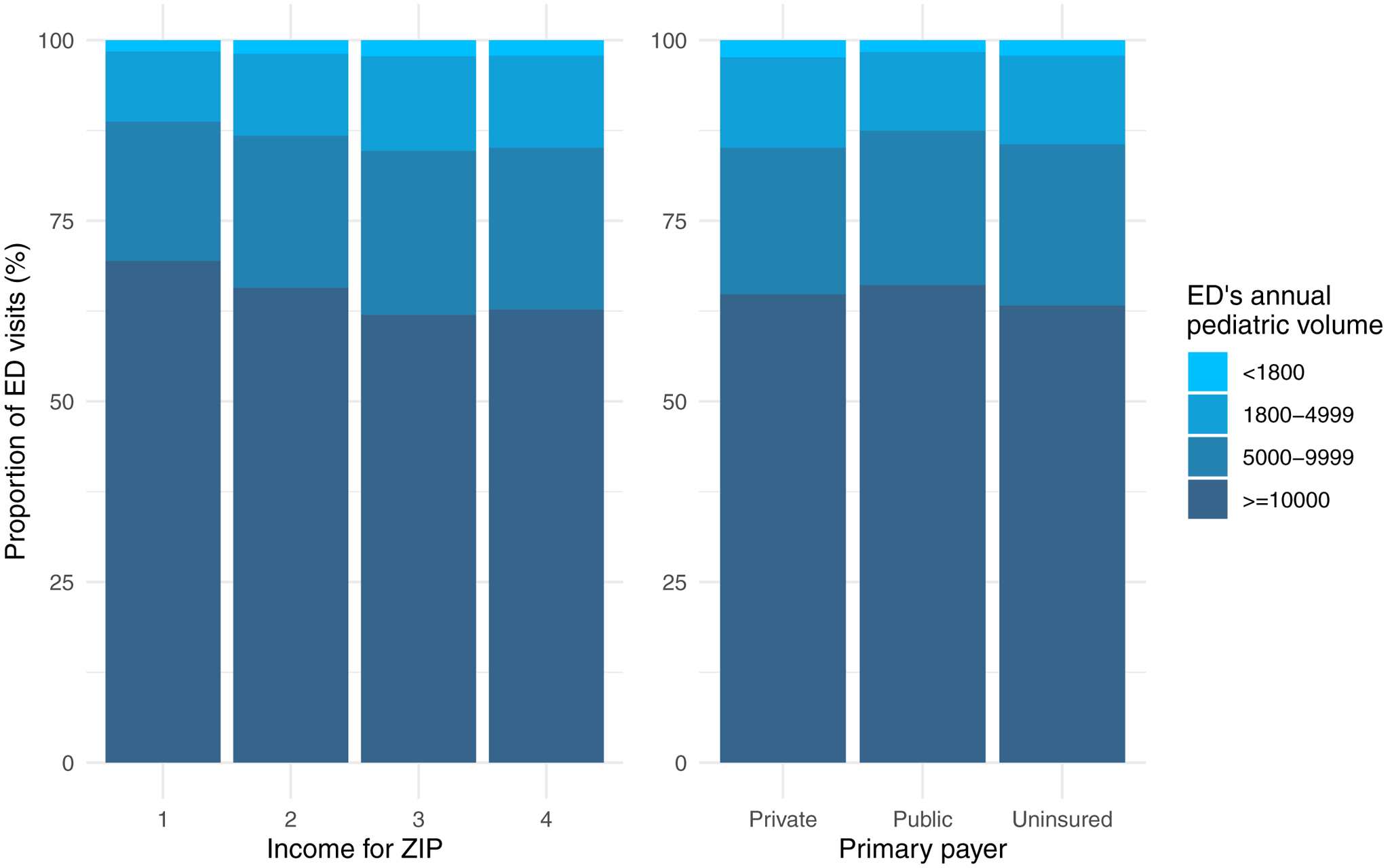
Of 107.6 million ED visits by children nationally from 2014 to 2017, children outside of the wealthiest neighborhood income quartile had lower proportions of visits to high-volume pediatric EDs (57.1% poorest quartile, 51.5% second, 56.6% third, 63.5% wealthiest) and greater proportions of visits to low-volume pediatric EDs (4.4% poorest, 6.4% second, 4.6% third, 2.3% wealthiest) than children in the wealthiest quartile. Adjustment for patient-level factors, particularly urban-rural status, inverted this association, revealing that lower neighborhood income was independently associated with visiting higher-volume pediatric EDs. Publicly insured children were modestly more likely to visit higher-volume pediatric EDs than privately insured and uninsured children in both unadjusted and adjusted analyses.
Nationally, children in lower-income neighborhoods tended to receive care in pediatric EDs with lower volume, an association that appears principally driven by urban-rural differences in access to emergency care.
为儿童提供的紧急护理的结果因患者社会经济因素和急诊部(ED)特征而有所不同,包括儿科量。这些因素如何在儿童寻求紧急护理的模式中相互交叉尚不清楚。本研究的目的是描述儿童邻里收入和保险类型与他们接受护理的 ED 特征之间的全国性关联。
我们使用全国急诊部样本对 2014 年至 2017 年期间的儿童急诊就诊进行了横断面研究。我们确定了邻里收入和患者保险类型与按儿科量类别就诊的 ED 就诊比例之间的关联,包括居住的城乡状况在内的患者水平因素未调整和调整后。
2014 年至 2017 年期间,全国范围内有 1.076 亿儿童急诊就诊,收入不在最富裕邻里收入四分位区间的儿童到高容量儿科 ED 的就诊比例较低(最贫穷四分位的 57.1%,其次为 51.5%,第三为 56.6%,最富裕为 63.5%),到低容量儿科 ED 的就诊比例较高(最贫穷的 4.4%,其次为 6.4%,第三为 4.6%,最富裕为 2.3%),而最富裕四分位的儿童则较低。对患者水平因素的调整,特别是城乡状况,颠覆了这种关联,表明较低的邻里收入与就诊较高容量的儿科 ED 独立相关。在未调整和调整分析中,与私人保险和无保险的儿童相比,公共保险的儿童更有可能就诊于高容量的儿科 ED。
在全国范围内,收入较低社区的儿童往往在儿科量较低的 ED 就诊,这种关联主要是由于获得紧急护理的城乡差异所致。