Ahmed Jawad, Hasnain Nimra, Fatima Iayla, Malik Farheen, Chaudhary Muhammad A, Ahmad Junaid, Malik Mehreen, Malik Laraib, Osama Muhammad, Baig Mirza Zain, Khosa Faisal, Bhora Faiz
Internal Medicine, Dow University of Health Sciences, Karachi, PAK.
General Surgery, St. Luke's General Hospital, Killenny, IRL.
Cureus. 2020 Sep 16;12(9):e10491. doi: 10.7759/cureus.10491.
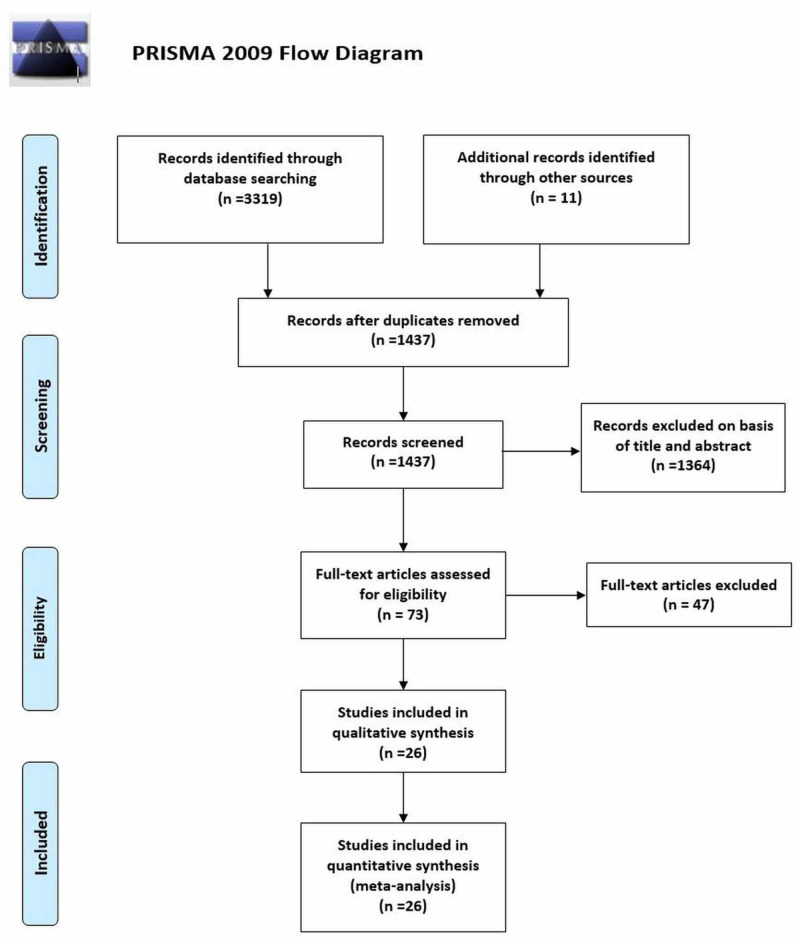
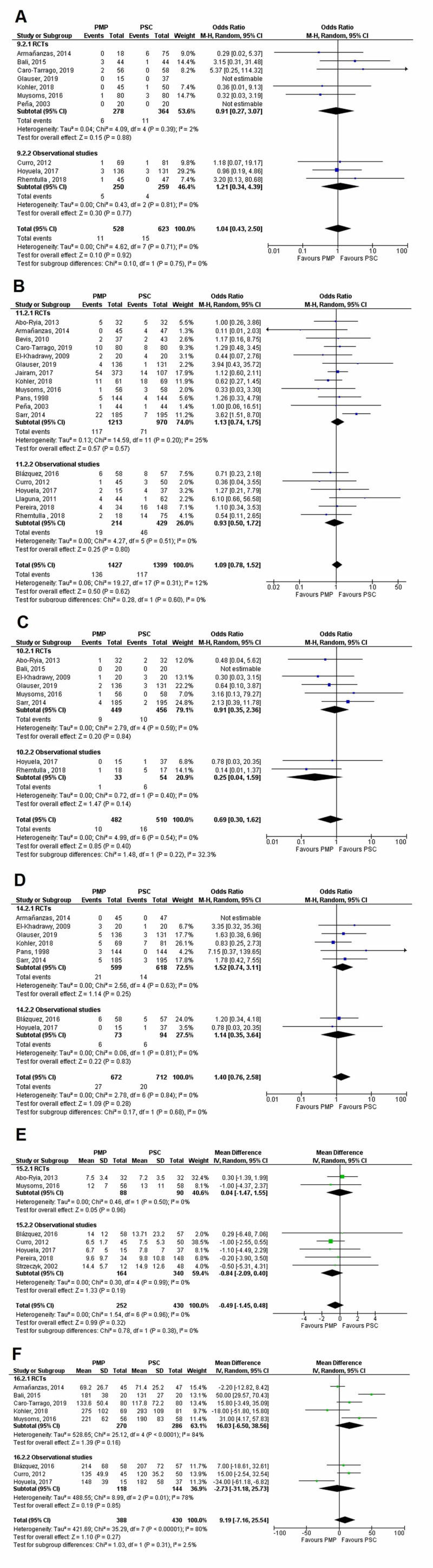
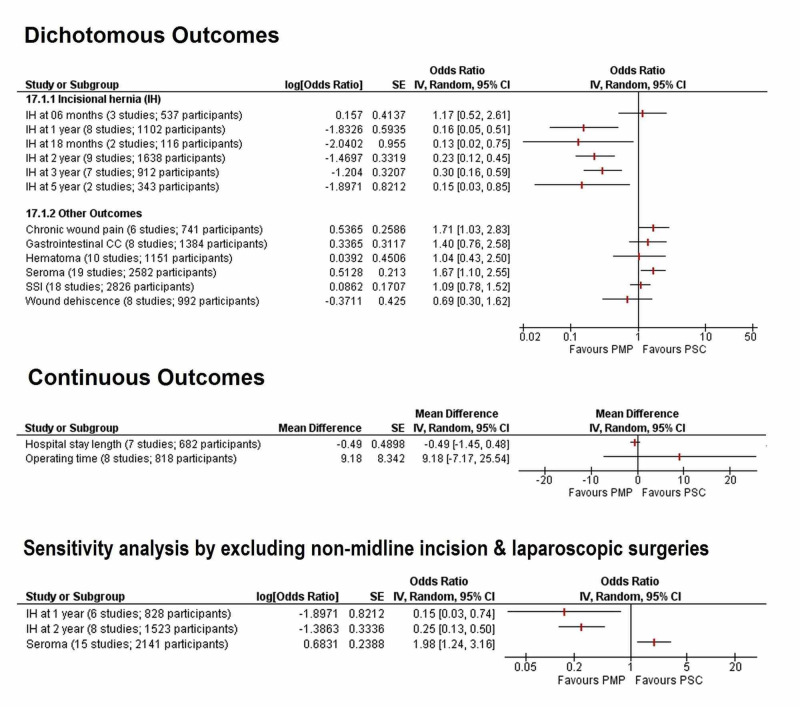
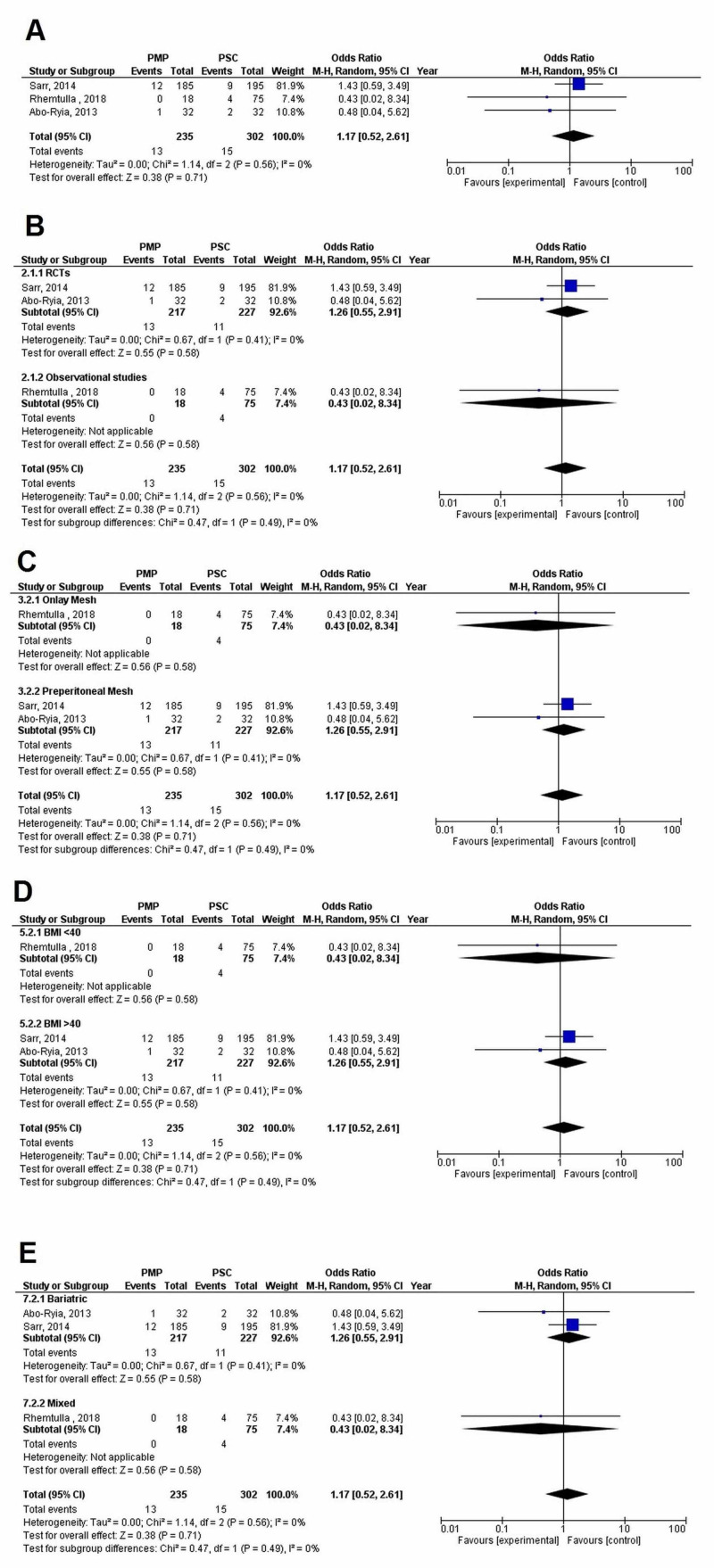
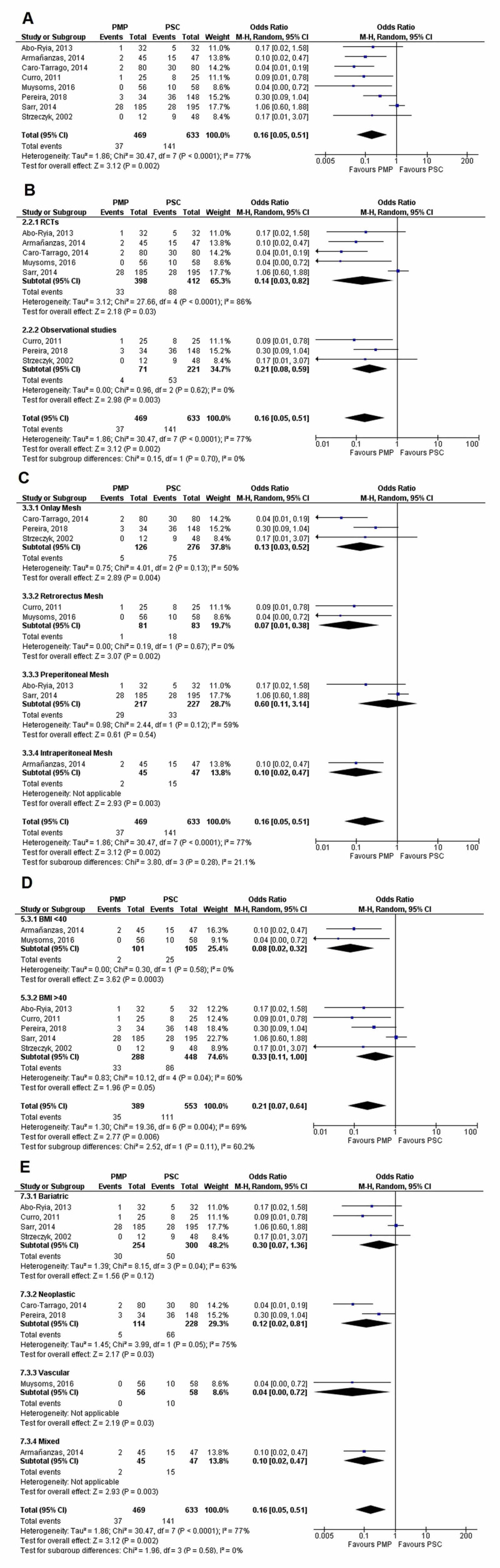
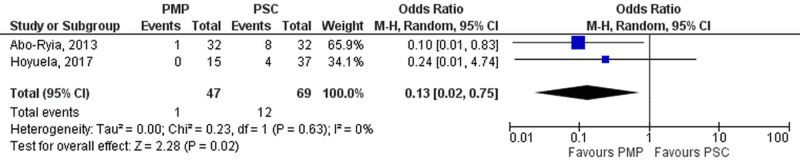
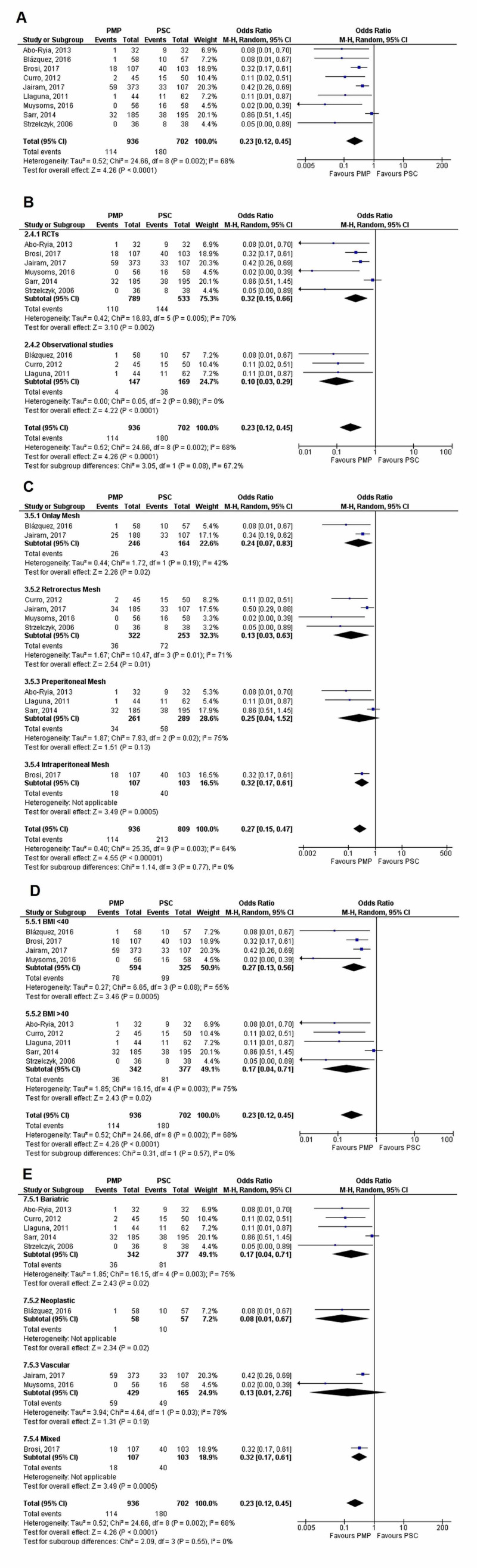
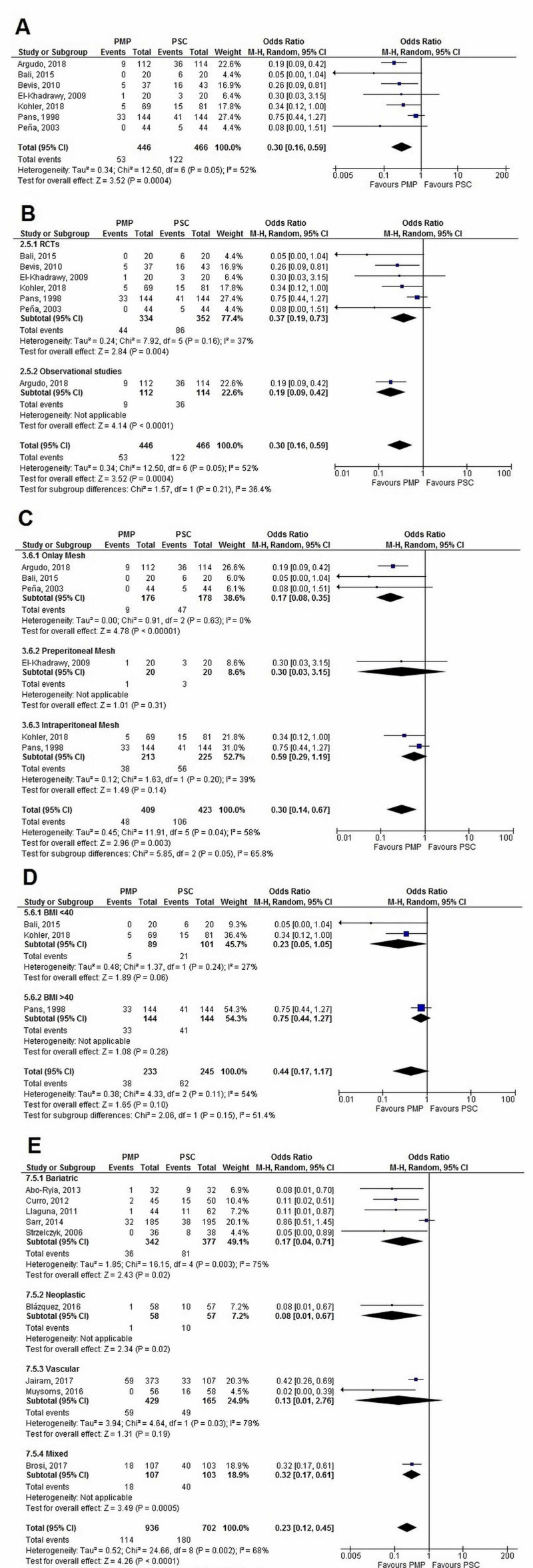
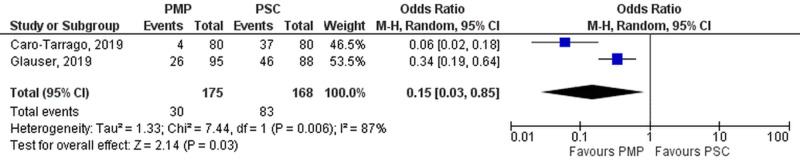
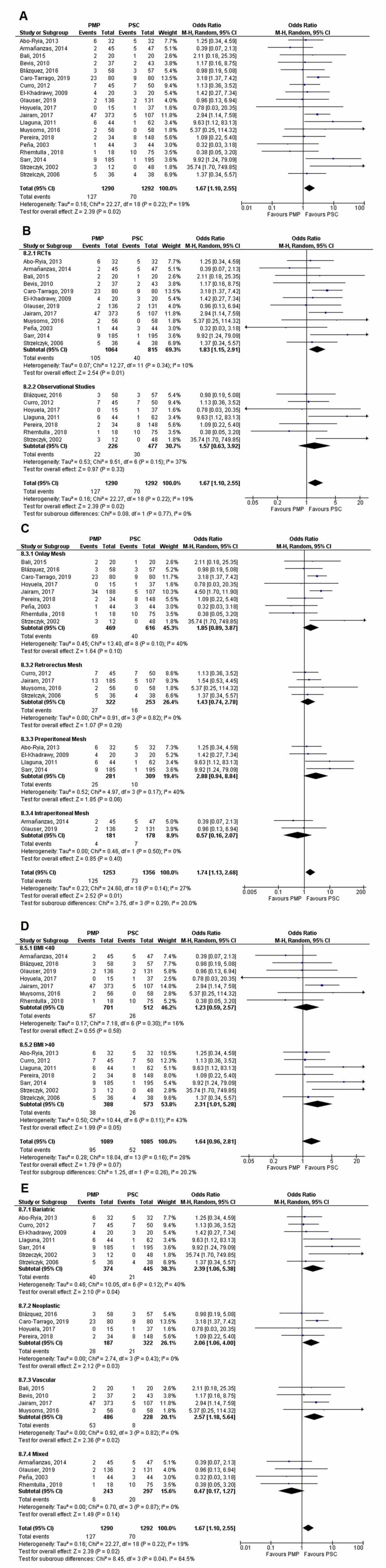
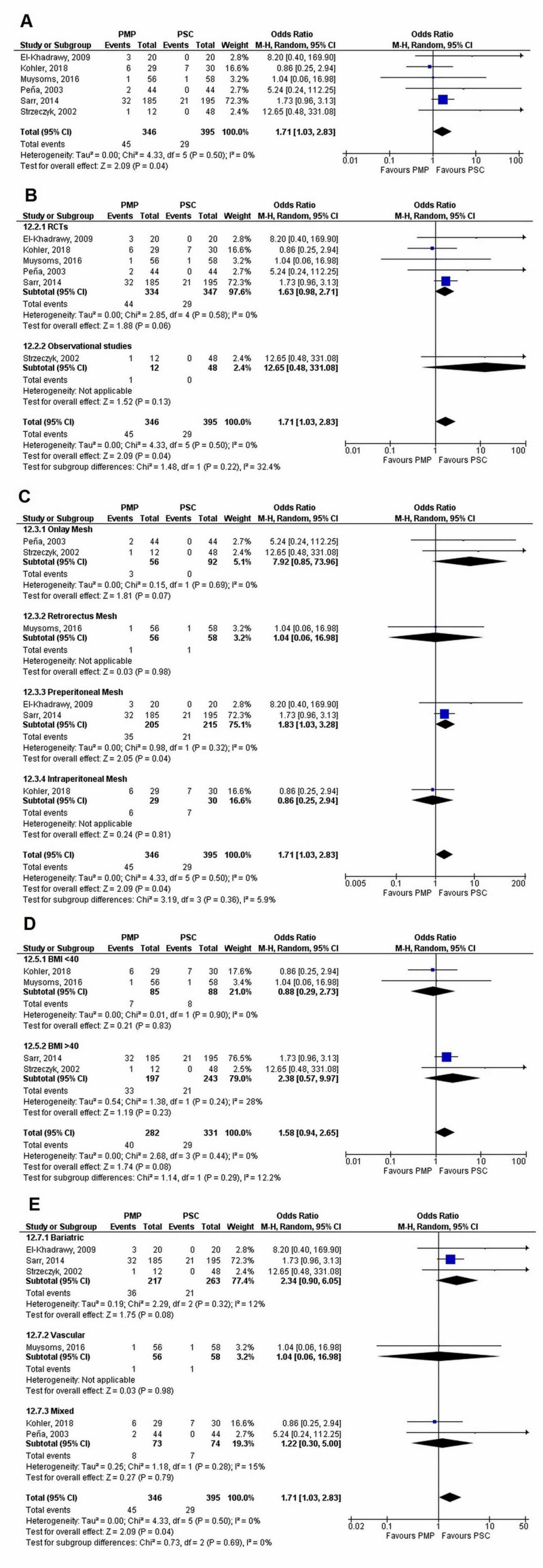
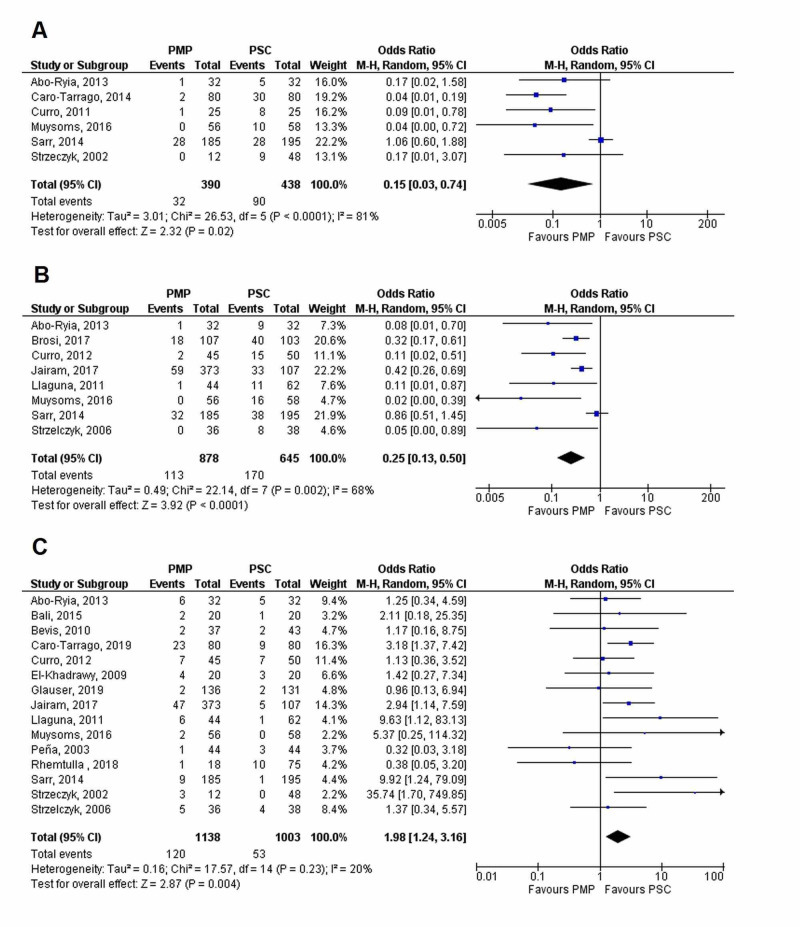
Background and objectives In high-risk populations, the efficacy of mesh placement in incisional hernia (IH) prevention after elective abdominal surgeries has been supported by many published studies. This meta-analysis aimed at providing comprehensive and updated clinical implications of prophylactic mesh placement (PMP) for the prevention of IH as compared to primary suture closure (PSC). Materials and methods PubMed, Science Direct, Cochrane, and Google Scholar were systematically searched until March 3, 2020, for studies comparing the efficacy of PMP to PSC in abdominal surgeries. The main outcome of interest was the incidence of IH at different follow-up durations. All statistical analyses were carried out using Review Manager version 5.3 (The Nordic Cochrane Centre, The Cochrane Collaboration, 2014) and Stata 11.0 (Stata Corporation LP, College Station, TX). The data were pooled using the random-effects model, and odds ratio (OR) and weighted mean differences (WMD) were calculated with the corresponding 95% confidence interval (CI). Results A total of 3,330 were identified initially and after duplicate removal and exclusion based on title and abstract, 26 studies comprising 3,000 patients, were included. The incidence of IH was significantly reduced for PMP at follow-up periods of one year (OR= 0.16 [0.05, 0.51]; p=0.002; I=77%), two years (OR= 0.23 [0.12, 0.45]; p<0.0001; I=68%), three years (OR= 0.30 [0.16, 0.59]; p=0.0004; I= 52%), and five years (OR=0.15 [0.03, 0.85]; p=0.03; I=87%). However, PMP was associated with an increased risk of seroma (OR=1.67 [1.10, 2.55]; p= 0.02; I=19%) and chronic wound pain (OR=1.71 [1.03, 2.83]; p= 0.04; I= 0%). No significant difference between the PMP and PSC groups was noted for postoperative hematoma (OR= 1.04 [0.43, 2.50]; p=0.92; I=0%), surgical site infection (OR=1.09 [0.78, 1.52]; p= 0.62; I=12%), wound dehiscence (OR=0.69 [0.30, 1.62]; p=0.40; I= 0%), gastrointestinal complications (OR= 1.40 [0.76, 2.58]; p=0.28; I= 0%), length of hospital stay (WMD= -0.49 [-1.45, 0.48]; p=0.32; I=0%), and operating time (WMD=9.18 [-7.17, 25.54]; p= 0.27; I=80%). Conclusions PMP has been effective in reducing the rate of IH in the high-risk population at all time intervals, but it is associated with an increased risk of seroma and chronic wound pain. The benefits of mesh largely outweigh the risk, and it is linked with positive outcomes in high-risk patients.
背景与目的 在高危人群中,许多已发表的研究支持在择期腹部手术后放置补片预防切口疝(IH)的有效性。本荟萃分析旨在提供与一期缝合关闭(PSC)相比,预防性补片放置(PMP)预防IH的全面且最新的临床意义。
材料与方法 系统检索PubMed、Science Direct、Cochrane和谷歌学术,直至2020年3月3日,以查找比较腹部手术中PMP与PSC疗效的研究。主要关注的结果是不同随访期IH的发生率。所有统计分析均使用Review Manager 5.3版(北欧Cochrane中心,Cochrane协作网,2014年)和Stata 11.0版(Stata公司,德克萨斯州大学城)进行。数据采用随机效应模型合并,并计算比值比(OR)和加权平均差(WMD)以及相应的95%置信区间(CI)。
结果 最初共识别出3330项研究,经重复文献去除及基于标题和摘要的排除后,纳入了26项研究,共3000例患者。在1年随访期(OR = 0.16 [0.05, 0.51];p = 0.002;I² = 77%)、2年随访期(OR = 0.23 [0.12, 0.45];p < 0.0001;I² = 68%)、3年随访期(OR = 0.30 [0.16, 0.59];p = 0.0004;I² = 52%)和5年随访期(OR = 0.15 [0.03, 0.85];p = 0.03;I² = 87%)时,PMP组的IH发生率显著降低。然而,PMP与血清肿风险增加相关(OR = 1.67 [1.10, 2.55];p = 0.02;I² = 19%)和慢性伤口疼痛风险增加相关(OR = 1.71 [1.03, 2.83];p = 0.04;I² = 0%)。PMP组与PSC组在术后血肿(OR = 1.04 [0.43, 2.50];p = 0.92;I² = 0%)、手术部位感染(OR = 1.09 [0.78, 1.52];p = 0.62;I² = 12%)、伤口裂开(OR = 0.69 [0.30, 1.62];p = 0.40;I² = 0%)、胃肠道并发症(OR = 1.40 [0.76, 2.58];p = 0.28;I² = 0%)、住院时间(WMD = -0.49 [-1.45, 0.48];p = 0.32;I² = 0%)和手术时间(WMD = 9.18 [-7.17, 25.54];p = 0.27;I² = 80%)方面未发现显著差异。
结论 PMP在所有时间间隔均有效降低高危人群的IH发生率,但与血清肿和慢性伤口疼痛风险增加相关。补片的益处远大于风险,且与高危患者的良好预后相关。