Long Wei-Guang, Cai Bin, Deng Jian-Ming, Liu Yang, Wang Wen-Jie, Luo Juan
Department of Chest Wall Surgery, Guangdong Second Provincial General Hospital, Guangzhou, China.
Transl Pediatr. 2020 Aug;9(4):551-560. doi: 10.21037/tp-20-199.
Chylothorax is a rare disease, defined as an abnormal accumulation of chylous lymphatic effusion in thoracic cavity, with a high mortality rate in pediatric patients. At present, there are few studies on the treatment of pediatric chylothorax, and conservative treatments like somatostatin (SST) and pleurodesis are performed empirically. SST has been used for treating pediatric chylothorax over 20 years, and povidone-iodine chemical pleurodesis (PICP) is adopted in recent years with a high cure rate, but both the effect are still uncertain. The safety and efficacy of SST and PICP in treating pediatric chylothorax was compared in this study.
From January 2009 to May 2020, 27 pediatric chylothorax patients who accepted life support, SST and PICP treatment were retrospectively reviewed in this study. Their medical history, clinical manifestations, pleural effusion examinations, treatment methods, effects, and complications were screened. PICP and SST was performed in 19 and 8 children, respectively. Each patient was followed up after discharge from the hospital.
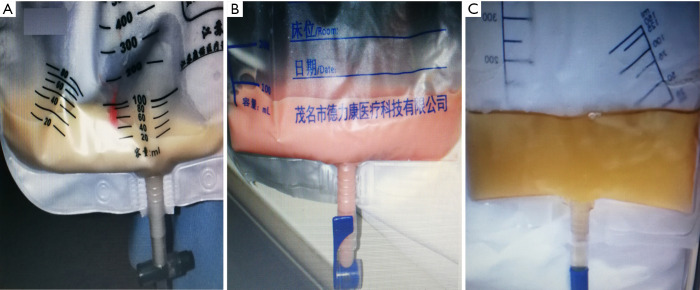
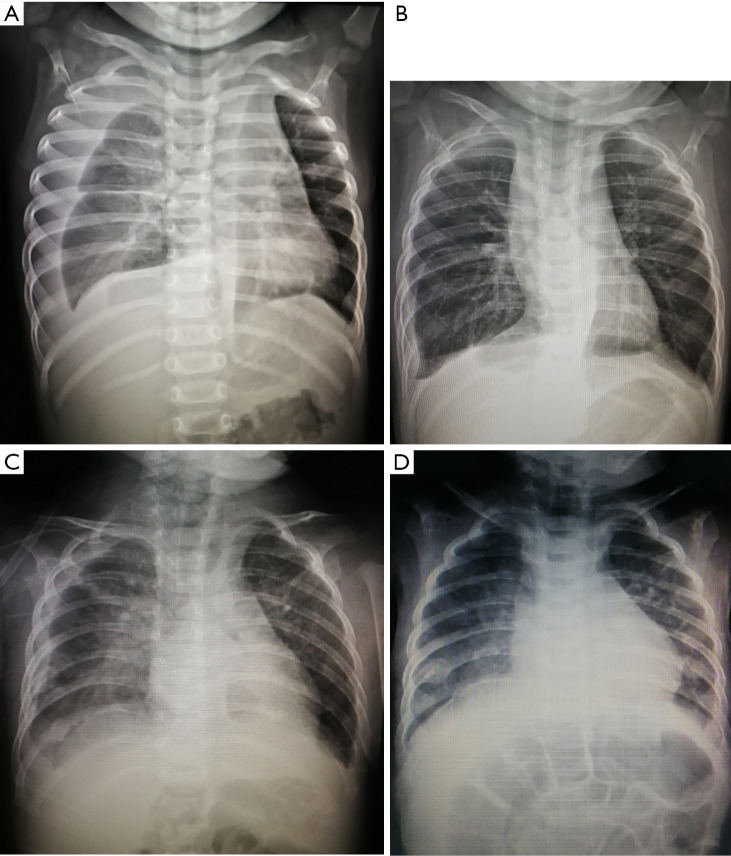
After admission, chest X-ray and ultrasound diagnosed pleural effusion in 27 patients (18 males and 9 females), including 13 and 6 cases on the left and right side, and 8 cases on both sides. In the pleural effusion, the mean leukocyte count was (9,826±9,482)×10/L, the mean lymphocyte ratio was (84.82±6.58)%, the mean triglyceride content was 7.11±6.63 mmol/L. In PICP and SST group, the mean length of stay was 38.42±19.42 and 35.13±12.72 d (P=0.664), the mean time of thoracic drainage was 24.58±16.34 and 19.63±8.88 d (P=0.440), the mean time of parenteral nutrition was 27.16±18.29 and 25.25±13.52 d (P=0.793), respectively. PICP was performed for 3.16±2.27 times, and SST was used for 14.75±9.08 d with the dosage of 0.5 to 10 µg/kg/hour. After the treatment, all patients in PICP group had mild chest pain and low-grade fever, and 12 cases were observed with transient decrease of oxygen saturation. Eight patients in SST group had nausea and vomit, and 1 child had diarrhea simultaneously. Both were cured by symptomatic treatment, thoracic drainage and discontinuing using SST. Three children were diagnosed with refractory chylothorax and cured by PICP after SST. Pleural effusion in 27 patients was finally absorbed. All of them achieved a clinical cure successfully, and there was no recurrence during discharge follow-up.
PICP has a high success rate and few adverse reactions in treating spontaneous chylothorax in pediatric patients, expected to be a new treatment option for pediatric chylothorax after SST.
乳糜胸是一种罕见疾病,定义为胸腔内乳糜性淋巴液异常积聚,在儿科患者中死亡率较高。目前,关于小儿乳糜胸治疗的研究较少,多经验性采用生长抑素(SST)及胸膜固定术等保守治疗方法。SST用于小儿乳糜胸治疗已20余年,近年来采用聚维酮碘化学胸膜固定术(PICP),治愈率较高,但两者疗效仍不确切。本研究比较SST与PICP治疗小儿乳糜胸的安全性及有效性。
回顾性分析2009年1月至2020年5月接受生命支持、SST及PICP治疗的27例小儿乳糜胸患者的病史、临床表现、胸腔积液检查、治疗方法、疗效及并发症。19例患儿行PICP治疗,8例患儿行SST治疗。所有患者出院后均进行随访。
入院后,胸部X线及超声检查确诊27例患者(男18例,女9例)存在胸腔积液,其中左侧13例,右侧6例,双侧8例。胸腔积液中,白细胞计数平均为(9,826±9,482)×10/L,淋巴细胞比例平均为(84.82±6.58)%,甘油三酯含量平均为7.11±6.63 mmol/L。PICP组与SST组平均住院时间分别为38.42±19.42天和35.13±12.72天(P = 0.664),胸腔引流平均时间分别为24.58±16.34天和19.63±8.88天(P = 0.440),肠外营养平均时间分别为27.16±18.29天和25.25±13.52天(P = 0.793)。PICP治疗3.16±2.27次,SST使用14.75±9.08天,剂量为0.5至10 μg/kg/小时。治疗后,PICP组所有患者均出现轻度胸痛及低热,12例患者出现氧饱和度短暂下降。SST组8例患者出现恶心、呕吐,1例患儿同时伴有腹泻。经对症治疗、胸腔引流及停用SST后均治愈。3例患儿诊断为难治性乳糜胸,经SST治疗后行PICP治愈。27例患者胸腔积液最终吸收。所有患者均成功临床治愈,出院随访期间无复发。
PICP治疗小儿自发性乳糜胸成功率高,不良反应少,有望成为继SST之后小儿乳糜胸的新治疗选择。