Fauer Alex, Wallner Lauren P, Davis Matthew A, Choi Sung Won, Friese Christopher R
University of Michigan, School of Nursing, Ann Arbor, MI, United States of America; University of Michigan, School of Public Health, Ann Arbor, MI, United States of America.
University of Michigan, Rogel Cancer Center, Ann Arbor, MI, United States of America; University of Michigan, Medical School, Ann Arbor, MI, United States of America; University of Michigan, School of Public Health, Ann Arbor, MI, United States of America.
J Geriatr Oncol. 2021 Mar;12(2):250-255. doi: 10.1016/j.jgo.2020.09.008. Epub 2020 Sep 20.
This study examined the association of ED use in the first year of diagnosis and patient experiences in care among older adults with hematologic malignancies.
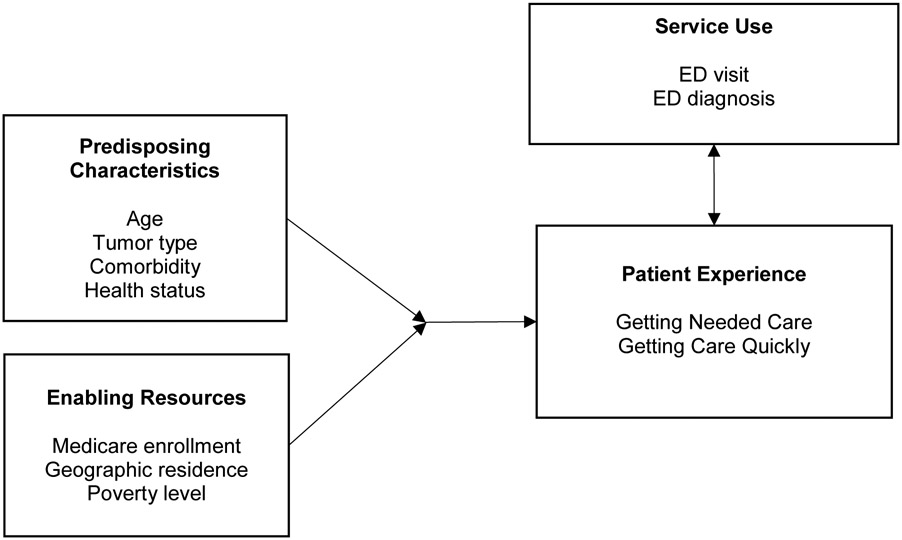
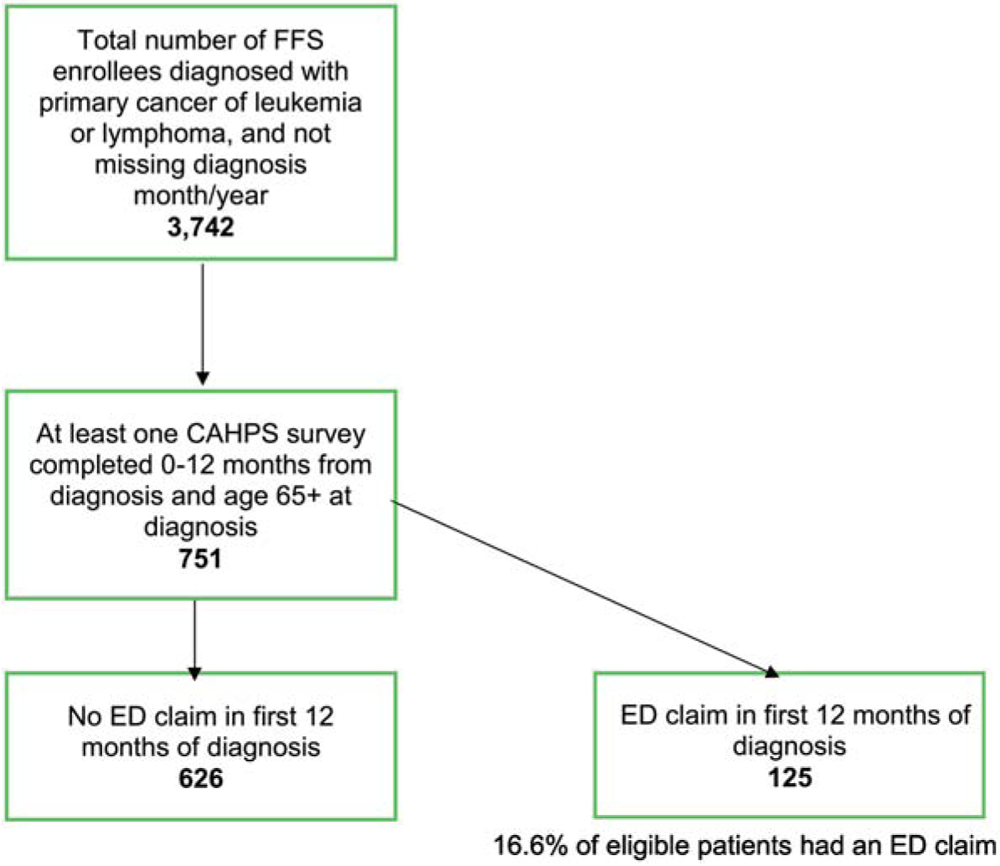
Cross-sectional design using SEER-CAHPS® data from 2002 to 2015 to study Medicare fee-for-service enrollees with a primary diagnosis of leukemia or lymphoma. We linked the CAHPS survey data (patient-reported experiences with health services) to patients' cancer registry information and Medicare outpatient claims from the SEER-CAHPS resource. We estimated associations of ED use and clinical characteristics with two CAHPS outcomes - "getting care quickly" (timeliness) and "getting needed care" (access) - with bivariate and multivariate analyses.
The analytic sample included 751 patients, 125 of whom had an ED claim in the first year of cancer diagnosis. The most frequent ED diagnosis clusters were fever and infection (n = 17, 13.6%), orthopedic and injury (16, 12.8%) and pain (16, 12.8%). Significantly more enrollees with an ED claim were diagnosed with lymphoma (p < 0.01), lived in rural areas (p < 0.01), and lived in areas with many families living in poverty (p < 0.01). In adjusted models, enrollees with an ED claim reported significantly worse access to care (β - 4.83; 95%CI -9.29,-0.38; p = 0.03).
The management of urgent care concerns for adults with hematologic malignancies remains an important clinical and quality improvement imperative. Further study is warranted to enhance the management of emergent complications in older adults receiving care for hematologic malignancies, with efforts that enhance coordination of ambulatory oncology care.
本研究探讨了老年血液系统恶性肿瘤患者确诊第一年的急诊使用情况与就医体验之间的关联。
采用横断面设计,利用2002年至2015年的SEER-CAHPS®数据,研究原发性诊断为白血病或淋巴瘤的医疗保险按服务收费参保者。我们将CAHPS调查数据(患者报告的医疗服务体验)与患者的癌症登记信息以及SEER-CAHPS资源中的医疗保险门诊索赔数据相链接。我们通过双变量和多变量分析估计了急诊使用情况和临床特征与两个CAHPS结果——“快速获得护理”(及时性)和“获得所需护理”(可及性)之间的关联。
分析样本包括751名患者,其中125人在癌症诊断的第一年有急诊索赔。最常见的急诊诊断类别是发热和感染(n = 17,13.6%)、骨科和损伤(16,12.8%)以及疼痛(16,12.8%)。有急诊索赔的参保者中,被诊断为淋巴瘤的比例显著更高(p < 0.01),居住在农村地区的比例显著更高(p < 0.01),且居住在贫困家庭较多地区的比例显著更高(p < 0.01)。在调整模型中,有急诊索赔的参保者报告的就医可及性显著更差(β - 4.83;95%CI -9.29,-0.38;p = 0.03)。
血液系统恶性肿瘤成人患者的紧急护理管理仍然是一项重要的临床和质量改进要务。有必要进一步开展研究,以加强接受血液系统恶性肿瘤护理的老年患者紧急并发症的管理,并努力加强门诊肿瘤护理的协调。