Department of Clinical Pharmacy and Pharmacology, University of Groningen, University Medical Centre Groningen, Groningen, The Netherlands.
School of Biomedical Sciences and Pharmacy, Faculty of Health and Medicine, University of Newcastle, Newcastle, NSW, Australia.
Diabet Med. 2021 Feb;38(2):e14408. doi: 10.1111/dme.14408. Epub 2020 Oct 2.
Individualizing goals for people with type 2 diabetes may result in deintensification of medication, but a comprehensive picture of deprescribing practices is lacking.
To conduct a scoping review in order to assess the rates, determinants and success of implementing deprescribing of glucose-, blood pressure- or lipid-lowering medications in people with diabetes.
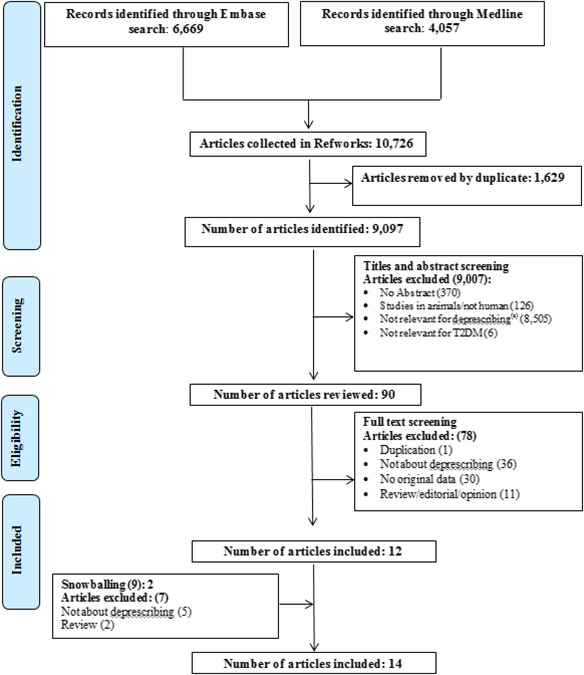
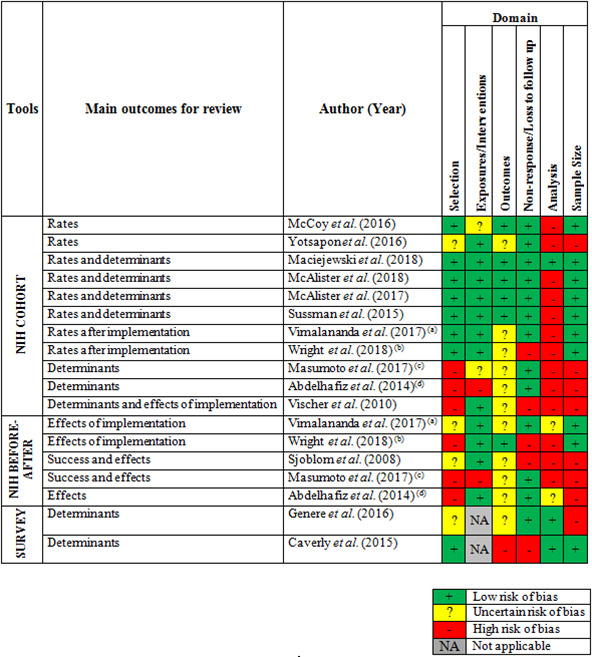
A systematic search on MEDLINE and Embase between January 2007 and January 2019 was carried out for deprescribing studies among people with diabetes. Outcomes were rates of deprescribing related to participant characteristics, the determinants and success of deprescribing, and its implementation. Critical appraisal was conducted using predefined tools.
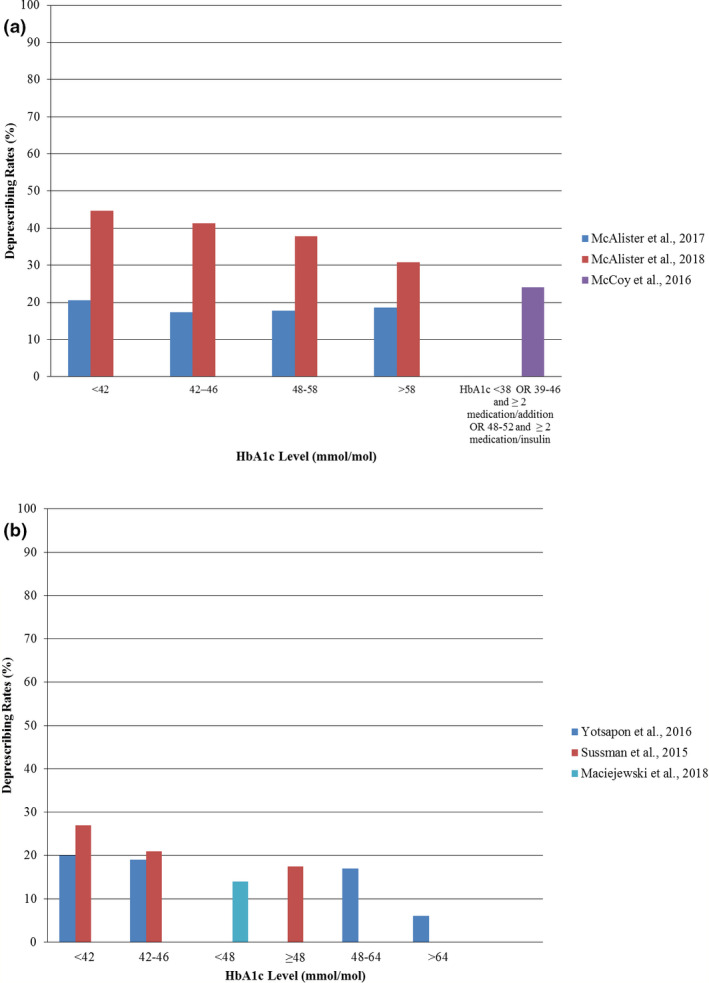
Fourteen studies were included; eight reported on rates, nine on determinants and six on success and implementation. Bias was high for studies on success of deprescribing. Deprescribing rates ranged from 14% to 27% in older people with low HbA levels, and from 16% to 19% in older people with low systolic blood pressure. Rates were not much affected by age, gender, frailty or life expectancy. Rates were higher when a reminder system was used to identify people with hypoglycaemia, which led to less overtreatment and fewer hypoglycaemic events. Most healthcare professionals accepted the concept of deprescribing but differed on when to conduct it. Deprescribing glucose-lowering medications could be successfully conducted in 62% to 75% of participants with small rises in HbA .
Deprescribing of glucose-lowering medications seems feasible and acceptable, but was not widely implemented in the covered period. Support systems may enhance deprescribing. More studies on deprescribing blood pressure- and lipid-lowering medications in people with diabetes are needed.
为 2 型糖尿病患者制定个体化目标可能导致药物治疗强度降低,但缺乏关于停药实践的全面描述。
进行范围综述,以评估在糖尿病患者中降低血糖、血压或血脂药物剂量的停药率、决定因素和实施成功率。
对 2007 年 1 月至 2019 年 1 月期间发表的关于糖尿病患者停药的研究进行了 MEDLINE 和 Embase 的系统检索。研究结果为与参与者特征相关的停药率、停药的决定因素和成功率,以及停药的实施情况。使用预先确定的工具进行了批判性评估。
共纳入 14 项研究,其中 8 项报告了停药率,9 项报告了停药的决定因素,6 项报告了停药的成功率和实施情况。关于停药成功率的研究存在较高的偏倚。在 HbA 水平较低的老年患者和收缩压较低的老年患者中,停药率为 14%-27%;在年龄较大、性别、虚弱或预期寿命方面,停药率受影响较小。当使用提醒系统来识别低血糖患者时,停药率更高,这导致了更少的过度治疗和更少的低血糖事件。大多数医疗保健专业人员接受了停药的概念,但在何时进行停药方面存在分歧。在 HbA 略有升高的患者中,降低血糖药物的停药成功率可达 62%-75%。
降低降糖药物剂量似乎是可行且可接受的,但在涵盖的时期内并未广泛实施。支持系统可能会增强停药的实施。需要更多关于在糖尿病患者中降低血压和血脂药物的停药研究。