Michalek Peter, Hatahet Sasha Benjamin, Svetlosak Martin, Margitfalvi Peter, Waczulikova Iveta, Trnovec Sebastian, Böhm Allan, Benacka Ondrej, Hatala Robert
Faculty of Medicine, Comenius University in Bratislava, Bratislava, Slovakia.
Faculty of Medicine, Slovak Medical University in Bratislava, Bratislava, Slovakia.
Front Physiol. 2020 Aug 31;11:1115. doi: 10.3389/fphys.2020.01115. eCollection 2020.
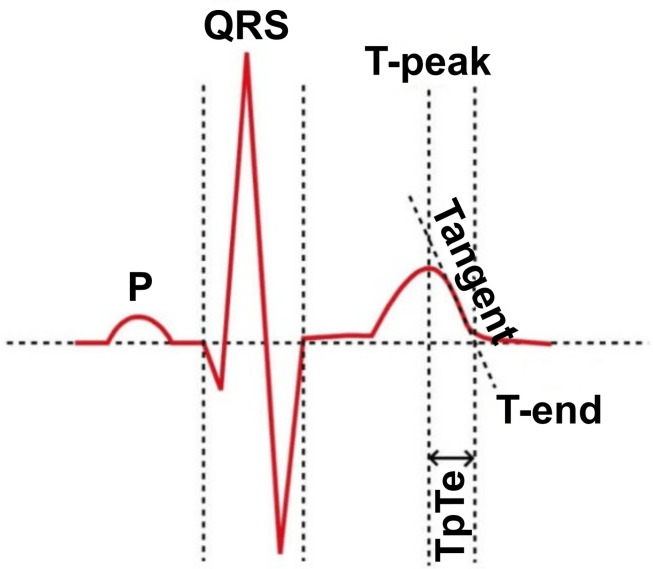
Potential of using the T-peak to T-end (TpTe) interval as an electrocardiographic parameter reflecting the transmural dispersion of ventricular repolarization (TDR) to identify patients (pts.) with higher risk of malignant ventricular arrhythmias (MVA) for better selection of candidates for implantable cardioverter-defibrillator (ICD) in primary prevention (PP) of sudden cardiac death (SCD) remains controversial. The primary objective of this study was to investigate the relationship between the TpTe interval in patient's preimplantation resting 12-lead electrocardiogram (ECG) and the incidence of MVA resulting in appropriate ICD intervention (AI). The secondary objective was to assess its relationship to overall mortality.
A total of 243 consecutive pts. with severe left ventricular (LV) systolic dysfunction after myocardial infarction (MI) with a single-chamber ICD for PP of SCD from one implantation center were included. Excluded were all pts. with any other disease that could interfere with the indication of ICD implantation. Primarily investigated intervals were measured manually in accordance with accepted methodology. Data on ICD interventions were acquired from device interrogation during regular outpatient visits. Survival data were collected from the databases of health insurance and regulatory authorities.
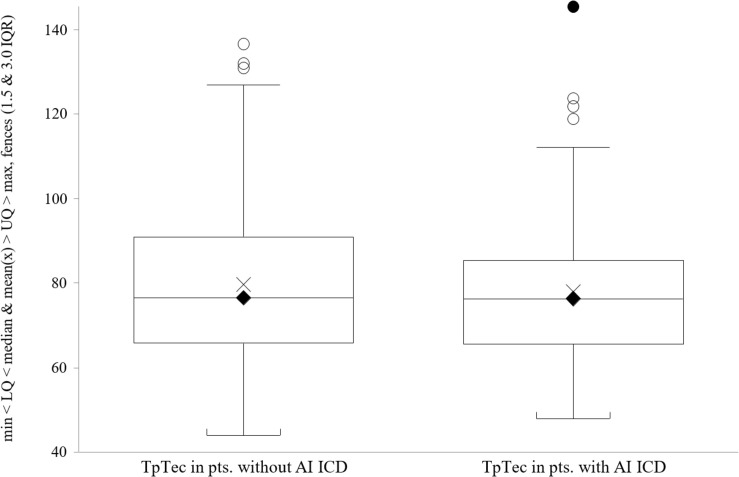
We did not find a significant relationship between the duration of the TpTe interval and the incidence of MVA (71.5 ms in pts. with MVA vs. 70 ms in pts. without MVA; = 0.408). Similar results were obtained for the corrected TpTe interval (TpTec) and the ratio of TpTe to QT interval (76.3 ms vs. 76.5 ms; = 0.539 and 0.178 vs. 0.181; = 0.547, respectively). There was also no significant difference between the duration of TpTe, TpTec and TpTe/QT ratio in pts. groups by overall mortality (71.5 ms in the deceased group vs. 70 ms in the survivors group; HR 1.01; 95% CI, 0.99-1.02; = 0.715, 76.3 ms vs. 76.5 ms; HR 1.01; 95% CI, 0.99-1.02; = 0.208 and 0.178 vs. 0.186; = 0.116, respectively).
This study suggests no significant association of overall or MVA-free survival with ECG parameters reflecting TDR (TpTe, TpTec) in patients with systolic dysfunction after MI and ICD implanted for primary prevention.
将T波峰至T波终末(TpTe)间期作为反映心室复极跨壁离散度(TDR)的心电图参数,以识别恶性室性心律失常(MVA)风险较高的患者,从而在心脏性猝死(SCD)一级预防(PP)中更好地选择植入式心律转复除颤器(ICD)候选者,其潜力仍存在争议。本研究的主要目的是调查患者植入前静息12导联心电图(ECG)中的TpTe间期与导致ICD恰当干预(AI)的MVA发生率之间的关系。次要目的是评估其与总死亡率的关系。
纳入来自一个植入中心的243例因心肌梗死(MI)后严重左心室(LV)收缩功能障碍而植入单腔ICD进行SCD一级预防的连续患者。排除所有患有可能干扰ICD植入指征的其他疾病的患者。主要研究的间期按照公认方法手动测量。ICD干预数据通过定期门诊随访时的设备问询获取。生存数据从医疗保险和监管机构的数据库中收集。
我们未发现TpTe间期时长与MVA发生率之间存在显著关系(发生MVA的患者为71.5毫秒,未发生MVA的患者为70毫秒;P = 0.408)。校正后的TpTe间期(TpTec)以及TpTe与QT间期的比值也得到了类似结果(分别为76.3毫秒对76.5毫秒;P = 0.539以及0.178对0.181;P = 0.547)。在按总死亡率分组的患者中,TpTe、TpTec和TpTe/QT比值的时长也无显著差异(死亡组为71.5毫秒,存活组为