Teyateeti Ajalaya, Mahvash Armeen, Long James P, Abdelsalam Mohamed E, Avritscher Rony, Chasen Beth, Kaseb Ahmed O, Kuban Joshua D, Murthy Ravi, Odisio Bruno C, Teyateeti Achiraya, Macapinlac Homer A, Kappadath S Cheenu
Department of Nuclear Medicine, Division of Diagnostic Imaging, University of Texas MD Anderson Cancer Center, Houston, TX, USA.
Division of Nuclear Medicine, Department of Radiology, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand.
J Hepatocell Carcinoma. 2020 Sep 14;7:117-131. doi: 10.2147/JHC.S248314. eCollection 2020.
To assess the overall survival (OS) and progression-free survival (PFS) of unresectable hepatocellular carcinoma (HCC) patients undergoing yttrium-90 glass-microsphere transarterial radioembolization (TARE) with and without concurrent sorafenib.
OS and PFS were analyzed in 55 patients with an intrahepatic tumor (IHT) ≤50% without advanced or aggressive disease features (ADFs), which was referred to presence of infiltrative/ill-defined HCC, macrovascular invasion, or extrahepatic disease treated with only TARE (TARE_alone) and in 74 patients with IHT ≤50% with ADFs or IHT >50% treated with TARE and sorafenib (TARE_sorafenib). Prognostic factors for OS and PFS were identified using univariate and multivariate analyses.
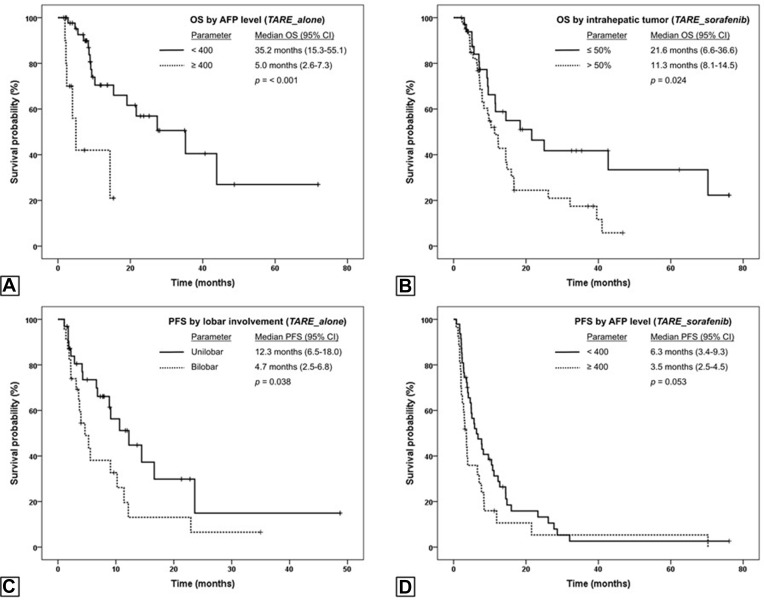
Median OS and PFS of TARE_alone patients were 21.6 (95% CI 6.1-37.1) and 9.1(95% CI 5.2-13.0) months, respectively, and for TARE_sorafenib patients 12.4 (95% CI 9.1-15.6) and 5.1 (95% CI 2.6-7.5) months, respectively. Better OS was associated with serum AFP <400 (HR 0.27, =0.02) in TARE_alone, and IHT ≤50% (HR 0.39, =0.004) and AFP <400 (HR 0.5, =0.027) in TARE_sorafenib. Unilobar involvement (HR 0.43, =0.029) and AFP <400 ng/mL (HR 0.52, =0.015) correlated with better PFS in TARE_alone and TARE_sorafenib, respectively. Adverse events (AEs) were more frequent in TARE_sorafenib than TARE_alone (92.4 vs 80.3%), but only 9.3% were grade 3 or higher AEs.
TARE_alone provided the most prominent survival benefit in IHT ≤50%-without ADF patients who had unilobar HCC and serum AFP <400 ng/mL. TARE and sorafenib yielded the best outcomes in patients with IHT ≤50% and serum AFP <400 ng/mL, with some additional grade 1-2 AEs compared to TARE only.
评估接受钇 - 90 玻璃微球经动脉放射性栓塞(TARE)联合或不联合索拉非尼治疗的不可切除肝细胞癌(HCC)患者的总生存期(OS)和无进展生存期(PFS)。
对 55 例肝内肿瘤(IHT)≤50% 且无进展期或侵袭性疾病特征(ADF)(即不存在浸润性/边界不清的 HCC、大血管侵犯或肝外疾病)仅接受 TARE 治疗(TARE_alone)的患者以及 74 例 IHT≤50% 伴有 ADF 或 IHT>50% 接受 TARE 和索拉非尼治疗(TARE_sorafenib)的患者的 OS 和 PFS 进行分析。使用单因素和多因素分析确定 OS 和 PFS 的预后因素。
TARE_alone 组患者的中位 OS 和 PFS 分别为 21.6(95%CI 6.1 - 37.1)个月和 9.1(95%CI 5.2 - 13.0)个月,TARE_sorafenib 组患者分别为 12.4(95%CI 9.1 - 15.6)个月和 5.1(95%CI 2.6 - 7.5)个月。在 TARE_alone 组中,血清 AFP<400 与更好的 OS 相关(HR 0.27,P = 0.02);在 TARE_sorafenib 组中,IHT≤50%(HR 0.39,P = 0.004)和 AFP<400(HR 0.5,P = 0.027)与更好的 OS 相关。单叶受累(HR 0.43,P = 0.029)和 AFP<400 ng/mL(HR 0.52,P = 0.015)分别与 TARE_alone 组和 TARE_sorafenib 组更好的 PFS 相关。TARE_sorafenib 组的不良事件(AE)比 TARE_alone 组更频繁(92.4% 对 80.3%),但只有 9.3% 为 3 级或更高等级的 AE。
对于 IHT≤50%、无 ADF、单叶 HCC 且血清 AFP<400 ng/mL 的患者,单纯 TARE 的生存获益最为显著。对于 IHT≤50% 且血清 AFP<400 ng/mL 的患者,TARE 联合索拉非尼效果最佳,与单纯 TARE 相比会增加一些 1 - 2 级 AE。