Neurochemistry Laboratory, Department of Clinical Chemistry, Amsterdam Neuroscience, Vrije Universiteit Amsterdam, Amsterdam UMC, Boelelaan 1117, 1081 HV, Amsterdam, The Netherlands.
Alzheimer Center Amsterdam, Department of Neurology, Amsterdam Neuroscience, Vrije Universiteit Amsterdam, Amsterdam UMC, Amsterdam, The Netherlands.
Alzheimers Res Ther. 2020 Sep 28;12(1):118. doi: 10.1186/s13195-020-00682-7.
Blood-based biomarkers for Alzheimer's disease (AD) might facilitate identification of participants for clinical trials targeting amyloid beta (Abeta) accumulation, and aid in AD diagnostics. We examined the potential of plasma markers Abeta, glial fibrillary acidic protein (GFAP) and neurofilament light (NfL) to identify cerebral amyloidosis and/or disease severity.
We included individuals with a positive (n = 176: 63 ± 7 years, 87 (49%) females) or negative (n = 76: 61 ± 9 years, 27 (36%) females) amyloid PET status, with syndrome diagnosis subjective cognitive decline (18 PET+, 25 PET-), mild cognitive impairment (26 PET+, 24 PET-), or AD-dementia (132 PET+). Plasma Abeta, GFAP, and NfL were measured by Simoa. We applied two-way ANOVA adjusted for age and sex to investigate the associations of the plasma markers with amyloid PET status and syndrome diagnosis; logistic regression analysis with Wald's backward selection to identify an optimal panel that identifies amyloid PET positivity; age, sex, and education-adjusted linear regression analysis to investigate associations between the plasma markers and neuropsychological test performance; and Spearman's correlation analysis to investigate associations between the plasma markers and medial temporal lobe atrophy (MTA).
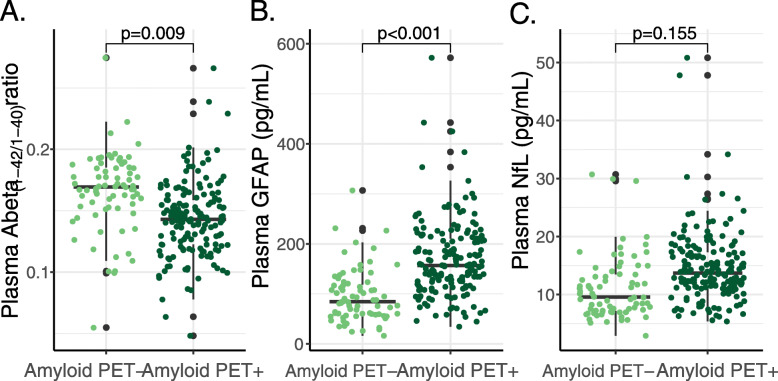
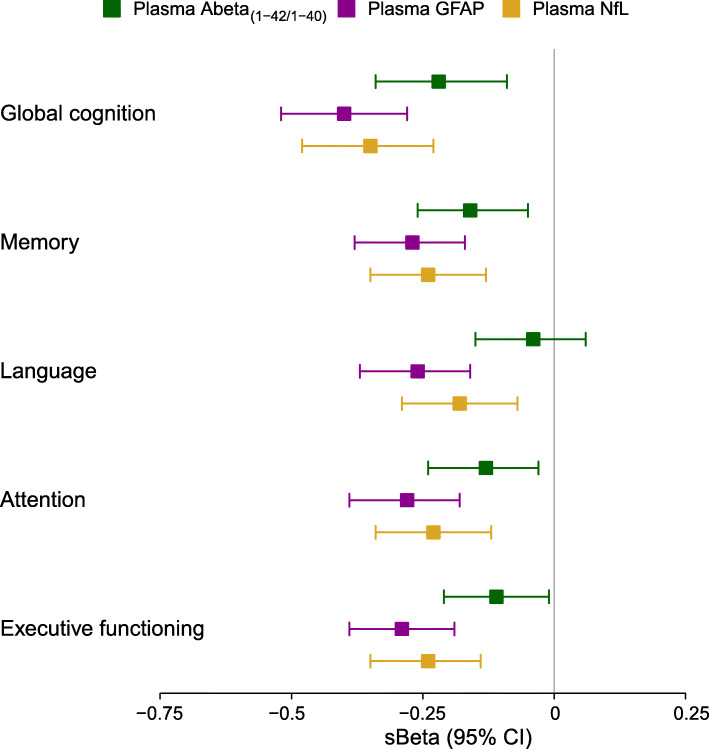
Abeta and GFAP independently associated with amyloid PET status (p = 0.009 and p < 0.001 respectively), and GFAP and NfL independently associated with syndrome diagnosis (p = 0.001 and p = 0.048 respectively). The optimal panel identifying a positive amyloid status included Abeta and GFAP, alongside age and APOE (AUC = 88% (95% CI 83-93%), 82% sensitivity, 86% specificity), while excluding NfL and sex. GFAP and NfL robustly associated with cognitive performance on global cognition and all major cognitive domains (GFAP: range standardized β (sβ) = - 0.40 to - 0.26; NfL: range sβ = - 0.35 to - 0.18; all: p < 0.002), whereas Abeta associated with global cognition, memory, attention, and executive functioning (range sβ = 0.22 - 0.11; all: p < 0.05) but not language. GFAP and NfL showed moderate positive correlations with MTA (both: Spearman's rho> 0.33, p < 0.001). Abeta showed a moderate negative correlation with MTA (Spearman's rho = - 0.24, p = 0.001).
Combination of plasma Abeta and GFAP provides a valuable tool for the identification of amyloid PET status. Furthermore, plasma GFAP and NfL associate with various disease severity measures suggesting potential for disease monitoring.
用于阿尔茨海默病(AD)的基于血液的生物标志物可能有助于鉴定针对淀粉样蛋白β(Abeta)积累的临床试验的参与者,并有助于 AD 的诊断。我们研究了血浆标志物 Abeta、神经胶质纤维酸性蛋白(GFAP)和神经丝轻链(NfL)识别脑淀粉样蛋白沉积和/或疾病严重程度的潜力。
我们纳入了具有阳性(n=176:63±7岁,87(49%)女性)或阴性(n=76:61±9岁,27(36%)女性)淀粉样蛋白 PET 状态的个体,综合征诊断为主观认知下降(18 例 PET+,25 例 PET-)、轻度认知障碍(26 例 PET+,24 例 PET-)或 AD 痴呆(132 例 PET+)。通过 Simoa 测量血浆 Abeta、GFAP 和 NfL。我们应用双因素方差分析调整年龄和性别,以研究血浆标志物与淀粉样蛋白 PET 状态和综合征诊断的关联;采用 Wald 后向选择的逻辑回归分析确定识别淀粉样蛋白 PET 阳性的最佳面板;采用年龄、性别和教育调整的线性回归分析研究血浆标志物与神经心理学测试表现之间的关联;以及采用 Spearman 相关分析研究血浆标志物与内侧颞叶萎缩(MTA)之间的关联。
Abeta 和 GFAP 独立与淀粉样蛋白 PET 状态相关(p=0.009 和 p<0.001),而 GFAP 和 NfL 独立与综合征诊断相关(p=0.001 和 p=0.048)。确定阳性淀粉样蛋白状态的最佳面板包括 Abeta 和 GFAP,以及年龄和 APOE(AUC=88%(95%CI 83-93%),82%的敏感性,86%的特异性),同时排除 NfL 和性别。GFAP 和 NfL 与认知表现的全球认知和所有主要认知领域密切相关(GFAP:范围标准化β(sβ)=-0.40 至-0.26;NfL:范围 sβ=-0.35 至-0.18;所有:p<0.002),而 Abeta 与全球认知、记忆、注意力和执行功能相关(范围 sβ=0.22-0.11;所有:p<0.05)但与语言无关。GFAP 和 NfL 与 MTA 呈中度正相关(两者:Spearman's rho>0.33,p<0.001)。Abeta 与 MTA 呈中度负相关(Spearman's rho=-0.24,p=0.001)。
Abeta 和 GFAP 的组合为鉴定淀粉样蛋白 PET 状态提供了有价值的工具。此外,血浆 GFAP 和 NfL 与各种疾病严重程度指标相关,表明其具有疾病监测的潜力。