Department of Neurology and the UAB Epilepsy Center, University of Alabama at Birmingham, Birmingham, Alabama, USA.
Department of Neurology, Rhode Island Hospital, Providence, Rhode Island, USA.
Ann Clin Transl Neurol. 2020 Oct;7(10):1973-1984. doi: 10.1002/acn3.51198. Epub 2020 Sep 29.
To further evaluate the relationship between the clinical profiles and limbic and motor brain regions and their connecting pathways in psychogenic nonepileptic seizures (PNES). Neurite Orientation Dispersion and Density Indices (NODDI) multicompartment modeling was used to test the relationships between tissue alterations in patients with traumatic brain injury (TBI) and multiple psychiatric symptoms.
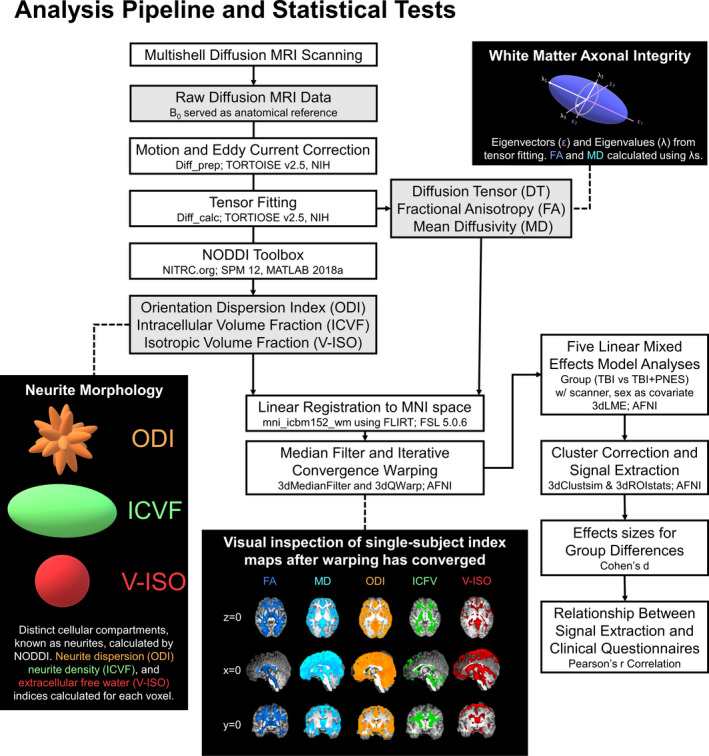
The sample included participants with prior TBI (TBI; N = 37) but no PNES, and with TBI and PNES (TBI + PNES; N = 34). Participants completed 3T Siemens Prisma MRI high angular resolution imaging diffusion protocol. Statistical maps, including fractional anisotropy (FA), mean diffusivity (MD), neurite dispersion [orientation dispersion index (ODI)] and density [intracellular volume fraction (ICVF), and free water (i.e., isotropic) volume fraction (V-ISO)] signal intensity, were generated for each participant. Linear mixed-effects models identified clusters of between-group differences in indices of white matter changes. Pearson's r correlation tests assessed any relationship between signal intensity and psychiatric symptoms.
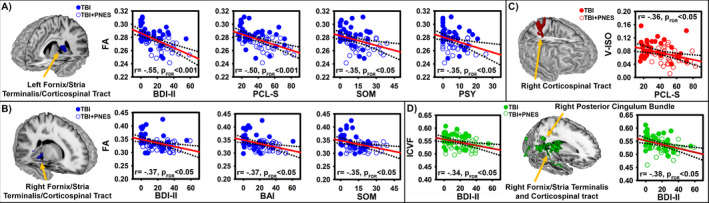
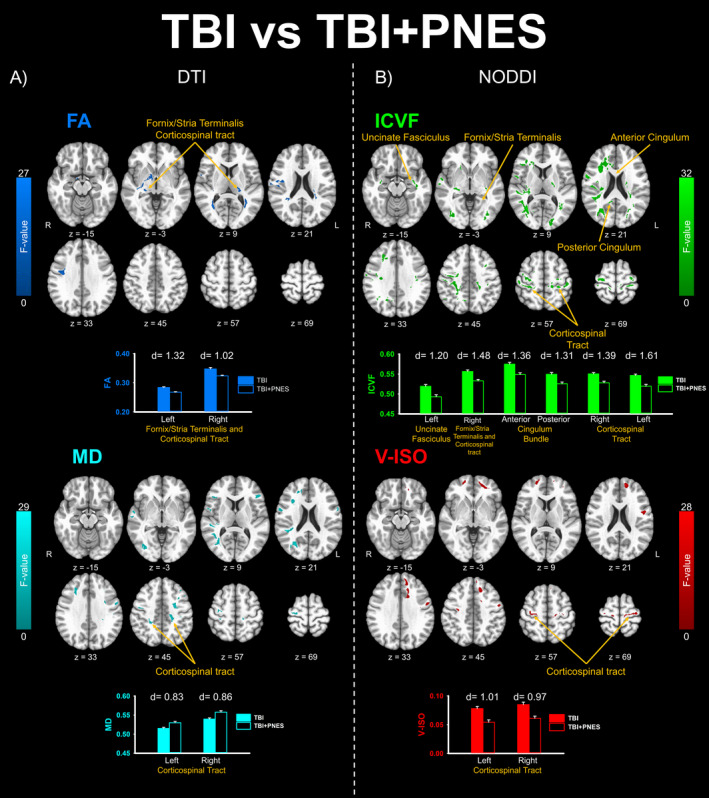
Compared to TBI, TBI + PNES revealed decreases in FA, ICVF, and V-ISO and increases in MD for clusters within cingulum bundle, uncinate fasciculus, fornix/stria terminalis, and corticospinal tract pathways (cluster threshold α = 0.05). Indices of white matter changes for these clusters correlated with depressive, anxiety, PTSD, psychoticism, and somatization symptom severity (FDR threshold α = 0.05). A follow-up within-group analysis revealed that these correlations failed to reach the criteria for significance in the TBI + PNES group alone.
The results expand support for the hypothesis that alterations in pathways comprising the specific PNES network correspond to patient profiles. These findings implicate myelin-specific changes as possible contributors to PNES, thus introducing novel potential treatment targets.
进一步评估心因性非癫痫性发作(PNES)患者的临床特征与边缘和运动脑区及其连接通路之间的关系。采用神经丝取向分散和密度指数(NODDI)多室模型来检验创伤性脑损伤(TBI)患者组织改变与多种精神症状之间的关系。
该样本包括既往有 TBI(TBI;N=37)但无 PNES 病史的参与者,以及 TBI 合并 PNES(TBI+PNES;N=34)的参与者。所有参与者均完成了 3T 西门子 Prisma MRI 高角度分辨率成像扩散方案。为每位参与者生成了包括各向异性分数(FA)、平均扩散系数(MD)、神经丝弥散[取向弥散指数(ODI)]和密度[细胞内容积分数(ICVF)和自由水(即各向同性)容积分数(V-ISO)]信号强度的统计图谱。线性混合效应模型确定了各组间白质改变指标的差异簇。Pearson r 相关检验评估了信号强度与精神症状之间的任何关系。
与 TBI 相比,TBI+PNES 显示在扣带束、钩束、穹窿/终纹、皮质脊髓束通路内的簇中 FA、ICVF 和 V-ISO 降低,MD 增加(簇阈值α=0.05)。这些簇的白质改变指数与抑郁、焦虑、创伤后应激障碍、精神病性和躯体化症状严重程度相关(FDR 阈值α=0.05)。一项后续的组内分析显示,这些相关性在 TBI+PNES 组中未能达到显著水平的标准。
这些结果进一步支持了这样的假设,即构成特定 PNES 网络的通路的改变与患者的特征相对应。这些发现表明髓鞘特异性改变可能是 PNES 的原因之一,从而引入了新的潜在治疗靶点。