UOC Ginecologia Oncologica, Dipartimento per la salute della Donna e del Bambino e della Salute Pubblica, Fondazione Policlinico Universitario A. Gemelli, IRCCS, Largo Agostino Gemelli 8, 00168, Rome, Italy.
Università Cattolica del Sacro Cuore, Largo Francesco Vito 1, 00168, Rome, Italy.
J Cancer Res Clin Oncol. 2021 Mar;147(3):649-659. doi: 10.1007/s00432-020-03393-6. Epub 2020 Sep 30.
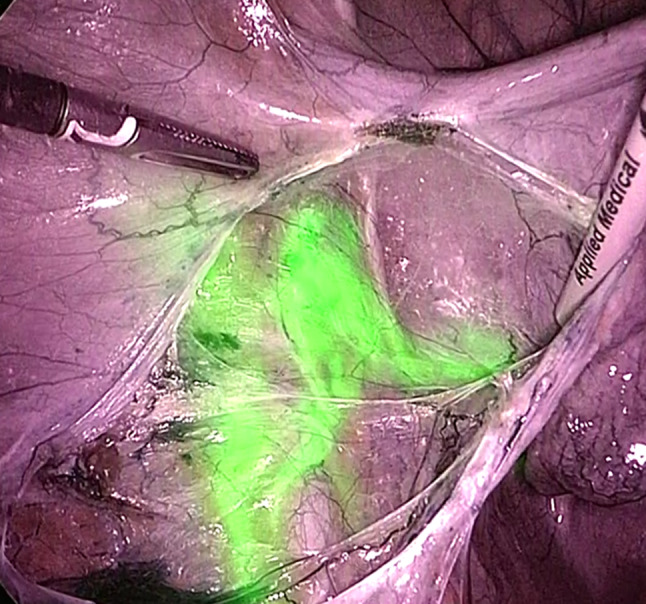
To assess the rate of bilateral sentinel lymph node (SLN) detection with indocyanine green (ICG), to evaluate the sensitivity and the negative predictive value of cervical cancer patients undergoing open radical hysterectomy; to compare open versus minimally invasive SLN biopsy performance and to assess factors related to no/unilateral SLN mapping.
We retrospectively reviewed consecutive patients with FIGO 2018 stage IA1 with lymph-vascular space involvement to IIB and IIIC1p cervical carcinoma who underwent SLN mapping with ICG followed by systematic pelvic lymphadenectomy between 05/2017 and 06/2020. Patients were divided according to surgical approach for statistical analysis.
Eighty-five patients met inclusion criteria. Twenty-seven (31.8%) underwent open and 58 (68.2%) underwent minimally invasive SLN mapping. No difference in any SLN mapping (laparotomy 92.6% and minimally invasive 91.4%) or in SLN bilateral detection (laparotomy 72.0% and minimally invasive 84.9%) (p = 0.850 and p = 0.222, respectively), in median number of SLNs mapped and retrieved (2 in both groups, p = 0.165) and in site of SLN mapping per hemi-pelvis (right side, p = 0273 and left side, p = 0.618) was evident between open and minimally invasive approach. Per-patient sensitivity of SLN biopsy in laparotomy was 83.3% (95% CI 35.9-99.6%) and the negative predictive value was 95.0% (95% CI 76.0-99.1%). No difference in per-patient sensitivity was noted between two approaches (p = 0.300). None of the analyzed variables was associated with no/unilateral SLN mapping.
The use of ICG to detect SLN in cervical cancer treated with open surgery allows a bilateral detection, sensitivity and negative predictive value comparable to minimally invasive surgery with potential advantages of ICG compared to other tracers.
评估使用吲哚菁绿(ICG)检测双侧前哨淋巴结(SLN)的比率,评估接受开腹根治性子宫切除术的宫颈癌患者的 SLN 活检的灵敏度和阴性预测值;比较开腹与微创 SLN 活检的性能,并评估与单侧或无 SLN 映射相关的因素。
我们回顾性分析了 2018 年FIGO 分期为 IA1 伴淋巴血管间隙浸润至 IIB 和 IIIC1p 宫颈癌的连续患者,这些患者于 2017 年 5 月至 2020 年 6 月期间接受了 ICG 引导的 SLN 映射,随后进行了系统的盆腔淋巴结清扫术。根据手术方法对患者进行了分组,以便进行统计分析。
85 名患者符合纳入标准。27 名(31.8%)接受了开腹 SLN 映射,58 名(68.2%)接受了微创 SLN 映射。任何 SLN 映射(剖腹术 92.6%和微创手术 91.4%)或 SLN 双侧检测(剖腹术 72.0%和微创手术 84.9%)(p=0.850 和 p=0.222)、中位数 SLN 映射和检索数量(两组均为 2 个,p=0.165)以及每半骨盆 SLN 映射的部位(右侧,p=0.273 和左侧,p=0.618)在开腹和微创方法之间没有差异。剖腹术 SLN 活检的患者灵敏度为 83.3%(95%CI 35.9-99.6%),阴性预测值为 95.0%(95%CI 76.0-99.1%)。两种方法之间的患者灵敏度无差异(p=0.300)。未发现任何分析变量与单侧或无 SLN 映射相关。
使用吲哚菁绿(ICG)检测开腹手术治疗的宫颈癌的 SLN 可实现双侧检测,灵敏度和阴性预测值与微创手术相当,与其他示踪剂相比,ICG 具有潜在优势。